
More Information
Submitted: March 10, 2026 | Accepted: March 30, 2026 | Published: March 31, 2026
Citation: Dragan A, Stan D, Zainea P, Voicu DC. Primary Ovarian Hydatid Cyst: Case Report and Review of the Literature. Clin J Obstet Gynecol. 2026; 9(1): 017-020. Available from:
https://dx.doi.org/10.29328/journal.cjog.1001201
DOI: 10.29328/journal.cjog.1001201
Copyright license: © 2026 Dragan A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Ovarian cyst; Echinococcosis; Ovarian hydatid cyst; Echinococcosis; Adnexal mass; Parasitic infection; Differential diagnosis

Primary Ovarian Hydatid Cyst: Case Report and Review of the Literature
A Dragan, Dorina Stan, Pusica Zainea and Dragoș Cristian Voicu*
County Emergency Clinical Hospital Braila, “Dunarea de Jos” University of Galati, Romania
*Corresponding author: Dragoș Cristian Voicu, County Emergency Clinical Hospital Braila, “Dunarea de Jos” University of Galati, Romania, Email: [email protected]
Background: Cystic echinococcosis is a zoonotic infection caused by Echinococcus granulosus, most commonly involving the liver and lungs. Ovarian localization is rare and may mimic benign or malignant adnexal masses, leading to diagnostic challenges.
Case presentation: We report the case of a 34-year-old woman from a rural area who presented with chronic pelvic pain and progressive abdominal distension. Imaging revealed a multilocular right ovarian cystic mass with internal daughter cysts. Tumor markers were within normal limits, while serology for echinococcosis was positive. The patient underwent right adnexectomy with careful intraoperative precautions to prevent spillage. Histopathological examination confirmed the diagnosis of ovarian hydatid cyst. Postoperative evolution was favorable under adjuvant albendazole therapy.
Conclusion: Ovarian hydatid cyst should be considered in the differential diagnosis of cystic adnexal masses, particularly in endemic regions. Accurate diagnosis and meticulous surgical management combined with antihelminthic therapy are essential to prevent recurrence and complications.
Cystic echinococcosis is a parasitic disease caused by the larval stage of Echinococcus granulosus. Humans become accidental intermediate hosts through ingestion of parasite eggs shed by definitive hosts, typically dogs. The liver (60% - 70%) and lungs (20% - 30%) are the most frequently involved organs [1].
Pelvic involvement is uncommon, and primary ovarian localization is exceptionally rare. When present, it may clinically and radiologically resemble benign ovarian cysts or ovarian malignancies, leading to delayed or incorrect diagnosis [2,3].
The present report describes a case of primary ovarian hydatid cyst and highlights diagnostic challenges, surgical management, and review of recent literature.
Patient information
A 34-year-old G2P2 woman from a rural area were presented with chronic intermittent pelvic pain (6 months duration), progressive abdominal distension, sensation of pelvic pressure. She also reported frequent contact with domestic animals (dogs and sheep). No fever, urinary, or gastrointestinal symptoms were noted. Menstrual cycles were regular.
Clinical findings
Physical examination revealed a palpable pelvic mass. Bimanual gynecologic examination identified a mobile right adnexal mass measuring approximately 8–9 cm.
Diagnostic assessment
Transvaginal ultrasound: Multilocular cystic mass of the right ovary with thin septations and multiple internal round structures suggestive of daughter cysts.
Computed Tomography (CT): Well-defined cystic lesion with internal daughter cysts, producing a honeycomb appearance (Figure 1A). No hepatic or pulmonary lesions were detected.
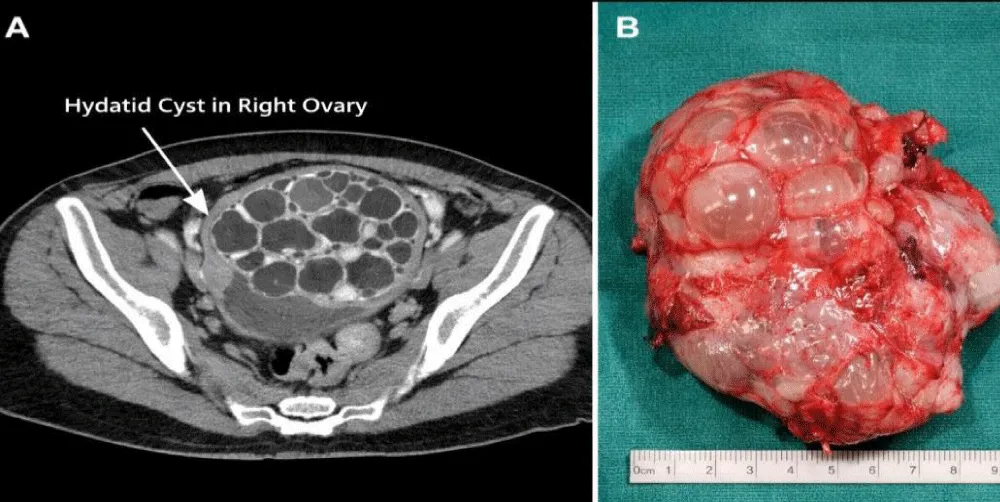
Figure 1: (A) CT scan showing a multilocular cystic lesion with daughter cysts producing a honeycomb appearance. (B) Macroscopic specimen of the ovarian cyst showing multiple daughter cysts filled with clear fluid.
Tumor markers: CA-125 within normal limits.
Serology: ELISA test positive for echinococcosis.
Based on imaging and epidemiological background, ovarian hydatid cyst was strongly suspected [2,4].
Therapeutic intervention
Exploratory laparotomy was performed. Intraoperatively, a well-encapsulated right ovarian cystic mass was identified. To prevent peritoneal dissemination, the operative field was protected with pads soaked in hypertonic saline.
Right adnexectomy was performed without rupture of the cyst. Macroscopic examination revealed multiple daughter cysts filled with clear fluid (Figure 1B).
Histopathological analysis confirmed the laminated membrane characteristic of hydatid cyst and the presence of protoscolices, establishing the definitive diagnosis.
Postoperatively, albendazole 400 mg twice daily was administered for three months in cyclic therapy, according to current recommendations [3,5].
Follow-up and outcomes
The postoperative course was uneventful. At 6- and 12-month follow-up, no evidence of recurrence was observed clinically or on imaging.
Ovarian hydatid cyst represents a rare manifestation of cystic echinococcosis. It may occur as: primary localization via hematogenous spread or secondary localization due to rupture of abdominal hydatid cysts [4].
Clinical manifestations are nonspecific and depend on cyst size and compression effects. Imaging plays a crucial role in diagnosis. The presence of daughter cysts and internal septations is highly suggestive [2,6].
The differential diagnosis should integrated clinical data and imaging features, in suggestive epidemiological context (residence in endemic areas, animal exposure).
Ovarian hydatid cyst
Clinical features: patients may be asymptomatic or present with nonspecific pelvic pain, abdominal distension, or a palpable mass.
Imaging: ultrasound and CT/MRI may show multiloculated cysts with daughter cysts (“wheel spoke” or “honeycomb” appearance), detached membranes (“water lily sign”), occasionally calcified cyst walls.
Functional/benign ovarian cysts ((e.g., follicular or corpus luteum cysts)
Clinical features: often asymptomatic, discovered incidentally; may cause mild cyclic pain.
Imaging: simple, unilocular, thin-walled cysts; anechoic content, no septations or solid components. Lack of internal architecture (no daughter cysts, no membranes) clearly differentiates them from hydatid disease.
Endometriomas (associated with endometriosis)
Clinical features: chronic cyclical pelvic pain, dysmenorrhea, infertility.
Imaging: homogeneous, low-level internal echoes (“ground-glass” appearance) on ultrasound; usually unilocular or mildly multilocular. Absence of daughter cysts and the characteristic “ground-glass” echotexture help distinguish endometriomas from hydatid cysts.
Mature cystic teratomas (dermoid cysts)
Clinical features: often asymptomatic; may present with mass effect or torsion.
Imaging: mixed cystic-solid lesion; presence of fat, calcifications, teeth, or hair (“tip of the iceberg” sign). The presence of fat and calcified elements is highly specific and not seen in hydatid cysts.
Malignant ovarian cystic tumors (e.g., epithelial ovarian carcinoma)
Clinical features: progressive abdominal distension, weight loss, ascites, systemic symptoms
Imaging: Complex cystic masses with thick septations, solid components or papillary projections, increased vascularity (on Doppler); often bilateral and associated with ascites.
Irregular solid elements, vascularity, and markedly elevated CA-125 strongly favor malignancy over hydatid disease.
Positive serology for echinococcosis may support diagnosis but is not definitive. Tumor markers are typically normal, helping differentiate from ovarian malignancy [3]. Although benign conditions (including inflammation or even hydatid cyst) can occasionally cause mild CA-125 elevations, they rarely produce high or persistent increases typical of malignancy. Moreover, when normal CA-125 levels are combined with non-suspicious imaging and clinical features, the overall probability of ovarian cancer becomes very low.
The designation of a primary ovarian hydatid cyst requires rigorous exclusion of more common sites of involvement (particularly the liver, spleen, and peritoneum), since ovarian localization is usually secondary.
Clarifying the diagnosis of a “primary” ovarian hydatid cyst presumes.
Preoperative imaging assessment
A comprehensive imaging workup is essential: abdominal ultrasound and contrast-enhanced CT/MRI should systematically evaluate the liver (most frequent site of hydatid disease), spleen, peritoneal cavity and omentum. In a true primary ovarian case, no cystic lesions are identified in hepatic or splenic parenchyma, no peritoneal implants, daughter cyst dissemination, or ascites suggestive of secondary spread. The ovarian lesion appears isolated, without evidence of contiguous or hematogenous dissemination.
Intraoperative findings and surgical exploration
Definitive confirmation often relies on careful intraoperative evaluation: systematic exploration of the abdominal cavity should be performed, including inspection and palpation of the liver surface and subhepatic space; examination of the spleen; evaluation of the entire peritoneum, omentum, mesentery, and pelvis.
In primary ovarian hydatid cyst: the lesion is confined to the ovary, with no additional cysts or peritoneal seedlings and no adhesions or rupture-related dissemination suggesting secondary implantation. The absence of synchronous lesions elsewhere strongly supports a primary origin.
Pathophysiological consideration
Primary ovarian involvement is thought to occur via hematogenous dissemination (bypassing hepatic and pulmonary filters) and less commonly by lymphatic spread.
This contrasts with secondary ovarian hydatidosis, which usually follows rupture or dissemination from hepatic or peritoneal cysts.
Laboratory findings (positive echinococcosis serology supports the parasitic etiology and normal CA-125 further reduces suspicion of malignancy, but does not distinguish primary vs. secondary hydatid disease)
This thorough exclusion of other sites is critical to avoid misclassification and to accurately report the rarity of primary ovarian involvement.
The treatment of choice is complete surgical excision without rupture, combined with perioperative antihelminthic therapy to reduce recurrence risk [5]. Inadequate management may lead to peritoneal dissemination or anaphylactic reactions.
Given the known risk of intraoperative hypersensitivity reactions associated with rupture of a hydatid cyst, specific prophylactic measures were implemented and clearly documented.
Prophylactic anti-allergic regimen
Preoperative pharmacologic prophylaxis is commonly used to reduce the risk and severity of anaphylaxis:
- Corticosteroids (e.g., intravenous hydrocortisone administered prior to incision);
- Antihistamines: both H1 (e.g., diphenhydramine) given 30–60 minutes before surgery;
This approach aims to blunt mast cell–mediated reactions in case of accidental cyst content spillage.
Intraoperative strict surgical precautions, in addition to pharmacologic prophylaxis
- Careful isolation of the operative field using pads soaked in scolicidal agents (e.g., hypertonic saline)
- Avoidance of cyst rupture through meticulous dissection
- Controlled aspiration of cyst contents when indicated and immediate suction and irrigation if spillage occurs.
- Continuous intraoperative monitoring (blood pressure, oxygen saturation, airway pressures); immediate availability of resuscitation drugs, especially epinephrine, as first-line treatment for anaphylaxis; preparedness for rapid fluid resuscitation and airway management.
Intraoperative and postoperative reactions
The report of intraoperative and postoperative reactions must explicitly mention:
- Whether cyst rupture occurred intraoperatively;
- Presence or absence of hypersensitivity reactions, such as: hypotension, bronchospasm, urticaria or rash
- Any need for emergency intervention (e.g., epinephrine administration)
Even if no adverse events were observed, this should be clearly noted (e.g., “No intraoperative anaphylactic or allergic reactions occurred”).
Recent systematic reviews emphasize the rarity of urogenital echinococcosis and highlight the need for awareness among gynecologists practicing in endemic areas [4].
Although rare, ovarian hydatid cyst should be included in the differential diagnosis of cystic adnexal masses, especially in patients from endemic rural regions.
Preoperative suspicion, careful surgical technique to avoid spillage, and adjunctive antihelminthic therapy (albendazole) are critical for optimal outcomes.
Greater awareness among gynecologists is necessary to prevent misdiagnosis and complications.
Ethical approval statement
This study was conducted in accordance with the ethical standards of the institutional research committee and with the Declaration of Helsinki. Ethical approval was obtained from the Institutional Ethics Committee of County Emergency Clinical Hospital Brăila, under approval number [protocol nr. 826 from 2024, august 26].
Informed consent statement
Written informed consent was obtained from the patient for participation in this study and for the publication of clinical data and images. A copy of the consent is available upon request.
Conflict of interest declaration: The authors declare that there are no conflicts of interest regarding the publication of this paper.
Funding statement: This research received no external funding.
Author contributions
Conceptualization: A.D, D.V.; Methodology: A.D., D.V.; Data Collection: D.S, P.Z.; Analysis: A.D.; Writing – Original draft: A.D.; Writing – Review & Editing: D.V.; Supervision: D.V. All authors have read and approved the final manuscript.
Data availability statement: The data supporting the findings of this study are available from the corresponding author upon reasonable request.
- Kumar K, Zaidi A, Husain N. Ovarian hydatid cyst: an uncommon site of presentation. Autopsy Case Rep. 2023;13:e2023383. Available from: https://doi.org/10.4322/acr.2023.461
- Hafsi M, Ragmoun H, Kristou E, Abaab A, Bezzine M. Hydatidosis in ovarian cysts: a case series and literature review. Int J Clin Obstet Gynaecol. 2025;9(3):B-38. Available from: https://doi.org/10.33545/gynae.2025.v9.i3b.1630
- Hezarjaribi HZ, Soleymani E, Ghahghaei-Nezamabadi A, Seifollahi A, Sharifi F, Montazeri M, et al. Challenges in diagnosing and managing ovarian hydatidosis: a case report and literature review from Iran. Acta Parasitol. 2025;70(6):237. Available from: https://doi.org/10.1007/s11686-025-01177-x
- Elmaslar Mert HT, Solak M, Sarı Serin P, Şakru N. Epidemiological and clinical characteristics of urogenital system cystic echinococcosis: a systematic review. Balkan Med J. 2025;42(6):506–515. Available from: https://doi.org/10.4274/balkanmedj.galenos.2025.2025-7-81
- Semash K, Voskanov M. Diagnostic challenges and treatment approaches for hydatid cysts in atypical localizations. World J Nephrol. 2025;14:107955. Available from: https://doi.org/10.5527/wjn.v14.i3.107955
- Ismail E, Dobrev P, Kovachev E, Anzhel S. Pelvic hydatid cyst in a female patient: case report and literature review. J Surg. 2026;11:11539. Available from: https://doi.org/10.29011/2575-9760.011539