
More Information
Submitted: February 20, 2024 | Approved: March 08, 2024 | Published: March 11, 2024
How to cite this article: Forlenza KN, Johansson AR, Onulack KW, McLoughlin RJ, Ulrich AP. Small Bowel Obstruction after Abdominal Myomectomy Involving Barbed Suture: A Case Report and Preventive Measures for Risk Reduction. Clin J Obstet Gynecol. 2024; 7: 034-036.
DOI: 10.29328/journal.cjog.1001160
Copyright License: © 2024 Forlenza KN, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Myomectomy; Barbed suture; V-loc; Small bowel obstruction; Laparoscopy; Postoperative complication

Small Bowel Obstruction after Abdominal Myomectomy Involving Barbed Suture: A Case Report and Preventive Measures for Risk Reduction
Kimberly N Forlenza1*, Alaina R Johansson2, Korey W Onulack1, Robert J McLoughlin2 and Amanda P Ulrich1
1Department of Obstetrics and Gynecology, University of Connecticut, Farmington, CT, USA
2Department of General Surgery, University of Connecticut, Farmington, CT, USA
*Address for Correspondence: Kimberly N Forlenza, MS, MD, Department of Obstetrics and Gynecology, University of Connecticut, Farmington, CT, USA, Email: [email protected]
In this report, we describe a case of a small bowel obstruction in the immediate postoperative period following an abdominal myomectomy. After failing conservative management, the patient underwent diagnostic laparoscopy, and the exposed tail of an absorbable barbed V-loc™ (Covidien™, Mansfield, MA, USA) suture used during the myomectomy was identified as the nidus of the small bowel obstruction. While barbed-suture-related bowel obstruction is a known rare complication that is well described in the general surgery literature, it is less documented in gynecological surgery literature. We anticipate the risk to be higher after multiple myomectomy, as postoperative contracture of the uterus can cause protrusion and exposure of the barbed suture tail. Though barbed suture can be safely used for hysterotomy closure during myomectomy, surgeons who opt to use barbed suture during myomectomy should be aware of this potential complication, take intra-operative measures to reduce the risk of postoperative tail protrusion and maintain a high index of suspicion for bowel obstruction in the immediate postoperative period.
A barbed suture is a surgical suture that features unidirectional barbs oriented in the opposite direction of the needle, which holds the suture in the tissue and prevents backsliding and loosening. The suture was first patented in 1964 and is now widely used in abdominal and gynecologic surgery [1,2]. One of its main advantages is that it avoids the need for laparoscopic knot tying, which requires a high level of skill and can present a barrier to minimally invasive approaches to surgery [2-4]. In gynecologic surgery, one of the common applications of barbed suture is the closure of hysterotomy incisions during myomectomies. When compared to conventional sutures, it has been shown to shorten the time it takes to close a uterine incision, as well as reduce blood loss and subsequent need for postoperative transfusion [5,6].
However, using a barbed suture is not without risk, as exposed barbed suture tails can cause bowel obstruction via mechanical obstruction and inflammation in the postoperative period. This complication is rare but well documented in abdominal and pelvic surgery literature, with cases reported after gastrectomy [7], gastric bypass [8], small and large bowel surgery [9], hernia repair [10], hysterectomy [11], pelvic organ prolapse surgery [12], and myomectomy [13]. Here, we present a case of barbed-suture-related small bowel obstruction after abdominal myomectomy, followed by some suggestions to mitigate this risk.
The patient is a 37-year-old G2P1102 female with a history of abdominal myomectomy via midline vertical incision sixteen years prior who presented with a recurrence of abnormal uterine bleeding. Pre-operative imaging demonstrated a recurrence of uterine leiomyomas. She underwent a repeat abdominal myomectomy via Pfannenstiel incision, and sixty uterine leiomyomas were removed. Absorbable 2 - 0 and 0 V-loc™ sutures were used for hysterotomy closure during the procedure. She developed nausea and failed to pass flatus by postoperative day two, and an imaging workup was initiated. CT scan demonstrated dilation of the small bowel with a transition point in the right lower quadrant, indicative of small bowel obstruction, and a nasogastric tube was placed on postoperative day three. She subsequently underwent a gastrografin challenge [14] on postoperative day five, in which contrast did not progress past the obstruction, representing a failure of conservative management. The decision was made to return to the operating room on postoperative day six for a diagnostic laparoscopy with General Surgery and Minimally Invasive Gynecologic Surgery. Given the multidisciplinary approach, the patient was placed in a dorsal lithotomy position and the abdomen and vagina were prepped in standard fashion. A uterine manipulator was placed to assist with the manipulation and identification of the obstruction.
Intraoperatively, numerous adhesions were visualized. Most notably, there was small bowel adherence to the tail of the V-loc™ suture that was used for hysterotomy closure on the posterior right cornua; this was assumed to be the obstruction point as the distal bowel loops appeared decompressed compared to the proximal loops. There was also adherence of the small bowel to the uterus in several additional locations on the posterior uterine corpus, which was suspected to be secondary to inflammation. Adhesions were taken down both bluntly and sharply, and the suture tail was trimmed. Seprafilm® slurry (Baxter International, Deerfield, IL, USA), a sterile hydrophilic adhesion barrier mixed with saline for laparoscopic application, was placed at the end of the case in an attempt to prevent future adhesions.
Images show the pre-operative uterus with multiple large leiomyomas on MRI (Figure 1), the bowel adhered to the V-loc™ suture on the posterior uterus at the lateral aspect of the hysterotomy closure (Figure 2), additional points of bowel adherence to the uterus (Figure 3), as well as the tail of the V-loc™ suture that was cut prior to the completion of the case (Figure 4).
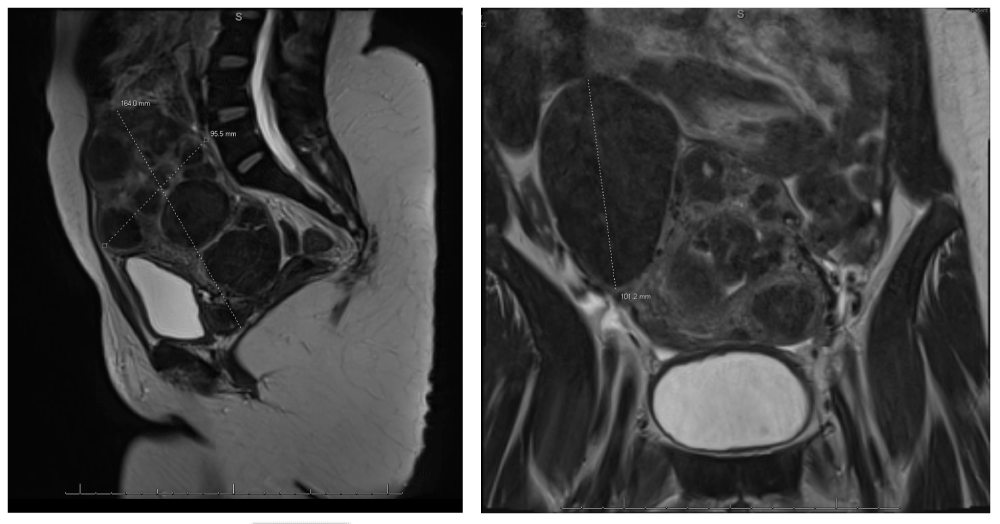
Figure 1: MRI imaging of pre-operative uterus with multiple large leiomyomas.
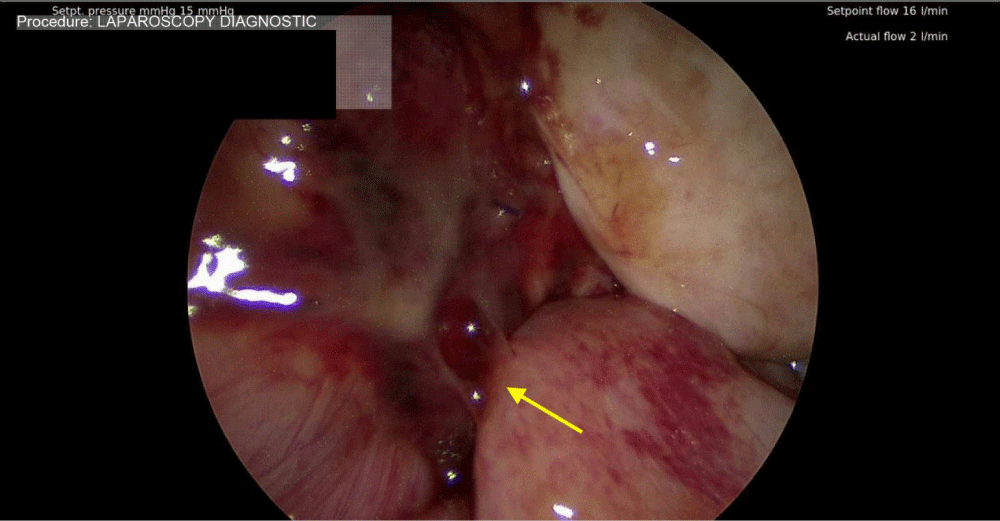
Figure 2: Point of bowel adherence to the V-loc™ suture.
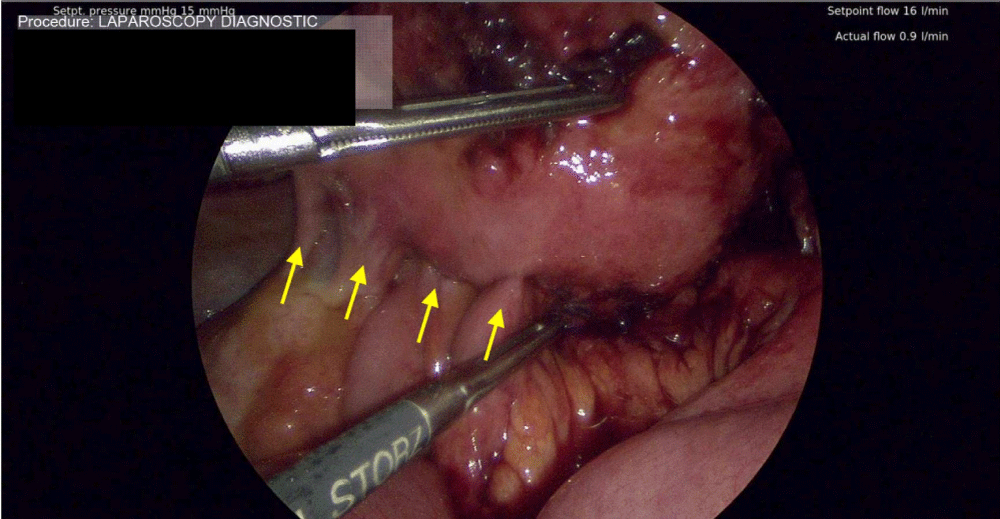
Figure 3: Additional bowel adhesions along the hysterotomy site.
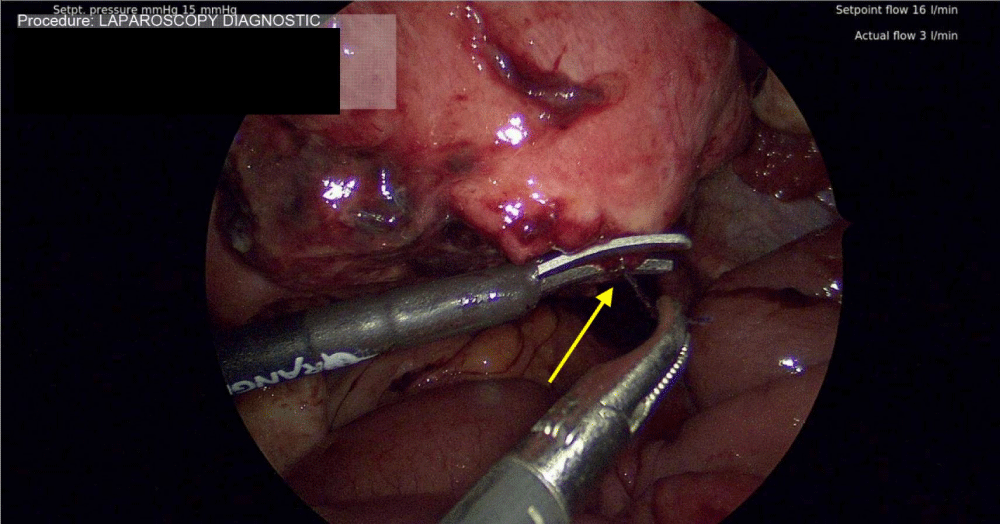
Figure 4: Trimming the exposed tail of the V-loc™ suture.
An exposed barbed suture presents a potential adhesion point that could lead to a small bowel obstruction. A 2021 review of all case reports of barbed-suture-related bowel obstruction over a 9-year period found myomectomy to be the second most common surgery associated with this complication (after hernia repair) [13]. This is likely due to the fact that the uterus undergoes post-myomectomy contracture around the hysterotomy site in the immediate postoperative period [13]; this contracture can cause protrusion of the barbed suture tail, thus conferring an elevated risk of tail exposure after myomectomy. The risk for our patient was high, given that sixty uterine leiomyomas were removed via multiple hysterotomy sites. Special care should be taken to prevent suture tail protrusion by cutting the tail as short as possible against the serosa [4,8,14]. As an additional precaution against tail protrusion, we recommend closing the serosa over the hysterotomy with a running baseball stitch to bury the tail and running the suture back one to two stitches in the opposite direction prior to cutting the suture to prevent suture slippage [13,15]. Finally, placing a physical barrier over the hysterotomy sites (such as oxidized regenerated cellulose sheets) may decrease surrounding inflammation and adhesion formation [4,13,15]. In this case report, given that re-operation occurred several days after the initial myomectomy, it was assumed that the uterus was fully contracted, and the suture tail was trimmed flush with the uterine wall to prevent further protrusion and obstruction.
Though barbed suture can be safely used for hysterotomy closure during myomectomy, it does carry the risk of postoperative small bowel obstruction. Surgeons who opt to use barbed suture during myomectomy should include this complication in the informed consent process, take intra-operative measures to reduce the risk of postoperative tail protrusion and maintain a high index of suspicion for bowel obstruction in the immediate postoperative period should the patient become symptomatic.
Ethical considerations
Verbal consent was obtained from the patient for this case report.
- Nambi Gowri K, King MW. A Review of Barbed Sutures-Evolution, Applications and Clinical Significance. Bioengineering (Basel). 2023 Mar 27;10(4):419. doi: 10.3390/bioengineering10040419. PMID: 37106607; PMCID: PMC10135495.
- Greenberg JA, Goldman RH. Barbed suture: a review of the technology and clinical uses in obstetrics and gynecology. Rev Obstet Gynecol. 2013;6(3-4):107-15. PMID: 24920976; PMCID: PMC4002186.
- Lim S, Ghosh S, Niklewski P, Roy S. Laparoscopic Suturing as a Barrier to Broader Adoption of Laparoscopic Surgery. JSLS. 2017 Jul-Sep;21(3):e2017.00021. doi: 10.4293/JSLS.2017.00021. PMID: 28694682; PMCID: PMC5491803.
- Bassi A, Tulandi T. Evaluation of total laparoscopic hysterectomy with and without the use of barbed suture. J Obstet Gynaecol Can. 2013 Aug;35(8):718-722. doi: 10.1016/S1701-2163(15)30862-8. PMID: 24007707.
- Ateş Tatar S, Karadağ B, Karadağ C, Duranoğlu Turgut G, Karataş S, Mülayim B. Barbed versus conventional suture in laparoscopic myomectomy: A randomized controlled study. Turk J Obstet Gynecol. 2023 Jun 1;20(2):126-130. doi: 10.4274/tjod.galenos.2023.21208. PMID: 37260187; PMCID: PMC10236233.
- Alessandri F, Remorgida V, Venturini PL, Ferrero S. Unidirectional barbed suture versus continuous suture with intracorporeal knots in laparoscopic myomectomy: a randomized study. J Minim Invasive Gynecol. 2010 Nov-Dec;17(6):725-9. doi: 10.1016/j.jmig.2010.06.007. Epub 2010 Jul 31. PMID: 20674510.
- Jang SH, Jung YK, Choi SJ, Ha TK. Postoperative mechanical small bowel obstruction induced by V-Loc barbed absorbable suture after laparoscopic distal gastrectomy. Ann Surg Treat Res. 2017 May;92(5):380-382. doi: 10.4174/astr.2017.92.5.380. Epub 2017 Apr 27. PMID: 28480186; PMCID: PMC5416918.
- Santucci W, Choy A, Cheng Q, Ward S, Winter N, Hii MW. Small bowel obstruction secondary to barbed sutures in bariatric surgery: a cautionary tale. ANZ J Surg. 2024 Feb 26. doi: 10.1111/ans.18892. Epub ahead of print. PMID: 38407555.
- Segura-Sampedro JJ, Ashrafian H, Navarro-Sánchez A, Jenkins JT, Morales-Conde S, Martínez-Isla A. Small bowel obstruction due to laparoscopic barbed sutures: an unknown complication? Rev Esp Enferm Dig. 2015 Nov;107(11):677-80. doi: 10.17235/reed.2015.3863/2015. PMID: 26541657.
- Tagliaferri EM, Wong Tavara SL, Abad de Jesus JL, Bergmann H, Hammans S, Seidlmayer CM. Small bowel obstruction SBO after TAPP repair caused by a self-anchoring barbed suture device for peritoneal closure: case report. J Surg Case Rep. 2018 Jul 20;2018(7):rjy165. doi: 10.1093/jscr/rjy165. PMID: 30046435; PMCID: PMC6054201.
- Donnellan NM, Mansuria SM. Small bowel obstruction resulting from laparoscopic vaginal cuff closure with a barbed suture. J Minim Invasive Gynecol. 2011 Jul-Aug;18(4):528-30. doi: 10.1016/j.jmig.2011.03.011. PMID: 21777845.
- Limbachiya D, Tiwari R, Kumari R, Aggarwal M. Barbed Suture Causing Acute Small Bowel Obstruction Post Laparoscopic Sacrocolpopexy. CRSLS. 2022 Nov 22;9(4):e2022.00058. doi: 10.4293/CRSLS.2022.00058. PMID: 36452882; PMCID: PMC9682608.
- Stabile G, Romano F, De Santo D, Sorrentino F, Nappi L, Cracco F, Ricci G. Case Report: Bowel Occlusion Following the Use of Barbed Sutures in Abdominal Surgery. A Single-Center Experience and Literature Review. Front Surg. 2021 Apr 20;8:626505. doi: 10.3389/fsurg.2021.626505. PMID: 33959630; PMCID: PMC8093862.
- Zielinski MD, Haddad NN, Cullinane DC, Inaba K, Yeh DD, Wydo S, Turay D, Pakula A, Duane TM, Watras J, Widom KA, Cull J, Rodriguez CJ, Toschlog EA, Sams VG, Hazelton JP, Graybill JC, Skinner R, Yune JM; EAST SBO Workgroup: Martin D. Zielinski, MD; Nadeem N. Haddad, MD; Asad J. Choudhry, MBBS; Daniel C. Cullinane, MD; Kenji Inaba, MD; Agustin Escalante; D. Dante Yeh, MD; Salina Wydo, MD; David Turay, MD; Andrea Pakula, MD; Therese M. Duane, MD; Jill Watras, MD; Kenneth A. Widom, MD; John Cull, MD; Carlos J. Rodriguez, DO; Eric A. Toschlog, MD; Valerie G. Sams, MD; Joshua P. Hazelton, DO; John Christopher Graybill, MD, Ruby Skinner, MD, Ji-Ming Yune, MD. Multi-institutional, prospective, observational study comparing the Gastrografin challenge versus standard treatment in adhesive small bowel obstruction. J Trauma Acute Care Surg. 2017 Jul;83(1):47-54. doi: 10.1097/TA.0000000000001499. PMID: 28422909.
- Wang L, Maejima T, Fukahori S, Nishihara S, Yoshikawa D, Kono T. Bowel obstruction and perforation secondary to barbed suture after minimally invasive inguinal hernia repair: report of two cases and literature review. Surg Case Rep. 2021 Jul 13;7(1):161. doi: 10.1186/s40792-021-01249-w. PMID: 34255201; PMCID: PMC8276904.