
More Information
Submitted: November 13, 2023 | Approved: December 01, 2023 | Published: December 04, 2023
How to cite this article: Zsoldos M, Pajor AK, Zsoldos K, Pusztafalvi H. Acceptance of Oral Sex among High School Students in Budapest: Incidence and Correlates. Clin J Obstet Gynecol. 2023; 6: 216-224.
DOI: 10.29328/journal.cjog.1001152
Copyright License: © 2023 Zsoldos M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Oral sex; Risk factors; High school students; Friends; Partner
Abbreviations: HPV: Human Papillomavirus

Acceptance of Oral Sex among High School Students in Budapest: Incidence and Correlates
Márta Zsoldos1, Attila K Pajor2* , Krisztián Zsoldos3 and Henriette Pusztafalvi4
, Krisztián Zsoldos3 and Henriette Pusztafalvi4
1University of Pécs, Faculty of Health Sciences, Doctoral School of Health Sciences, Pécs, Hungary
2Semmelweis University, Faculty of Medicine, Department of Obstetrics and Gynecology, Budapest, Hungary
3Dél-Buda Education District Centre, Budapest, Hungary
4University of Pécs, Faculty of Health Sciences, Department of Health Development and Public Health, Pécs, Hungary
*Address for Correspondence: Dr. Attila K Pajor, MD, DSc, Semmelweis University, Department of Obstetrics and Gynecology, 1082 Budapest, Üllöi ut 78 / A, Hungary, Email: [email protected]
Introduction: Adolescents and young adults often engage in oral sex. However, the factors affecting the development of agreeing with oral sex are not clear enough.
Objective: We aimed to assess the degree of agreement with oral sex among high school students and to search for background factors affecting this.
Material and method: We conducted a quantitative cross-sectional study among 157 females and 38 male high school students over the age of eighteen by using an anonymous, paper-based, multiple-choice, self-administered questionnaire. For statistical analysis, we used descriptive statistics, two-sample t-tests, and Spearman rank correlation.
Results: Of the respondents 67.9% were sexually active and 31.6% of them had more than one sexual partner. Of males 97.1% and of females 84.9% agreed with accepting oral sex. Degree of agreement with oral sex was higher in those who had had partnered sexual experience, and in those females who more frequently met close friends outside of school. Most participants were not in a current relationship with a partner, and for those who were, its duration did not affect the degree of accepting oral sex. The degree of agreement with the proficiency in male sexuality, and the degree of agreement with those dimensions of sexuality that most expressed the sexual drive and the desire to gratify it with the partner showed the strongest positive correlation with the degree of agreement with oral sex. In addition, the degree of agreement with the items of expressing sexual openness showed correlations with the degree of accepting oral sex.
Conclusion: The degree of agreement with oral sex is high among high school students. Among the factors influencing this, the intensity of meeting friends seems to be important. We therefore recommend that the schools improve sex education in groups, highlighting the risks of oral sex, to reach the target individuals and their friends as well as their potential partners.
Adolescents and young adults who engage in oral sex report being motivated in oral sex because they do have not to worry about pregnancy while acquiring partnered sexual pleasure and experience without using a condom, can satisfy their sexual curiosity and desire, can maintain their virginity, and they improve the emotional quality of their partnership as well as they need not be committed to a partner [1-4]. In addition, oral sex is often combined with vaginal intercourse to increase sexual arousal and to facilitate the orgasm in their partner [5].
Young people engaging in oral sex believe the risk of sexually transmitted infections to be low compared to vaginal sex, so they are not motivated in using a condom and do not or only very rarely use a condom to protect themselves during oral sex [6,7]. Therefore, sexually transmitted infections, especially human immunodeficiency virus infections more common occur after oral sex compared to vaginal intercourse just because of the rare use of a condom [8]. According to the HBSC study [9] the first sexual intercourse occurred in 45,2%, and 34,9% at the age of 15 years, and in 19.9% at the age of 16 years or later, furthermore, the last time when adolescents had sexual intercourse, they did not use a condom in at least 34.4%. In Hungary, one-third of adolescents don’t use condoms at all and an additional one-quarter don’t use it consistently in their sexual relationships [10]. Among sexually transmitted infections the Human Papillomavirus (HPV) infection appears to be the most common in Hungary because HPV infection of the uterine cervix was detected in 62.9% of women aged 15 - 25 applying for gynecological screening [11].
HPV is transmitted through both oral and vaginal sex. During oral sex, components of the partners' oral- and genital-related microbiomes are mixed with each other [12]. The heterosexual or homosexual partners may pass on their anaerobic bacteria and HPV from the oral microbiome into the vagina or to the penis, which can elicit bacterial vaginosis after the pathogens have colonized there [13]. Bacterial vaginosis is not a sexually transmitted infection but rather a syndrome involving changes in the microbiome of the vagina, which is characterized by a reduced rate of lactobacilli and by the diversity and predominance of anaerobic bacteria [14]. Research shows that both bacterial vaginosis and persistent HPV infection increase the risk of preterm birth [15,16]. In Hungary, the prevalence of preterm birth is around 9%, which causes a public health problem primarily in terms of perinatal morbidity and mortality [17].
It has been demonstrated that Hungarian high school students' knowledge about transmitting HPV is poor [18], and more than 40% of Polish university students aged 19 - 25 are unaware that oral sex can cause oral cancer in the long term [19]. Yet, in the U.S. oral sex among undergraduate students is the most common type of partnered sexual activity [20].
Considering that oral sex without using a condom has severe potential consequences such as bacterial vaginosis and preterm birth [14], that the lay public is mostly unaware of the links between oral sex and developing oral cancer [21, 22], and that over the past decade, the proportion of females reporting oral sex with a male partner has increased and the condom use at oral sex has decreased [23], it seems important to search for factors that can influence the degree of agreement with oral sex. The present study aimed to assess the rate of agreement with oral sex among high school students over eighteen years whose sexual attitudes have already developed, and to search for background factors that can affect the degree of agreement with oral sex. We hypothesized that the development of agreeing with oral sex is influenced by gender, sexual experience, duration of partner relationship, number of friends, frequency of meeting friends outside of school, and some components of sexual attitudes. So, we planned to examine the correlations of these factors with the extent of accepting oral sex.
Sampling
Budapest, the capital of Hungary, has 23 districts. From these, we randomly selected a central district, namely the 11th district, to examine the sexual attitudes of students attending state-run high schools. The district had four state-run high schools. One of them was an art high school at which students received full-time training after graduation for one year or two years. We planned to include all students over the age of 18 at the four high schools. Management of three institutions contributed to the survey. We visited all students over the age of 18 at these schools in the presence of their class teacher. We invited them to participate in our study and informed them that our research was aimed at learning about their lifestyle and sexual attitudes and that their responses to the questionnaire would be treated anonymously in coded form and as aggregated data. The head of the research and the class teachers emphasized that completing the questionnaires was voluntary and did not entail any advantages or disadvantages and it was not mandatory to respond to all questions. 197 students accepted the invitation to the study and finally, 195 were present at the school when the questionnaires were completed in the classroom during the class teacher's lesson.
Data collection
As a data collection method, we used a self-edited, multiple-choice, anonymous, paper-based, self-completed questionnaire which included demographic data, items of the peer and partner relationships, and sexual experiences and attitudes. Students completed the questionnaire in the classroom during the head teacher's lesson while the study leader was present. After completing the questionnaires, the study leader took them away together with the signed consent declarations of the students from the schools and then each questionnaire was numbered. Responses to the items of questionnaires were coded and uploaded to the Microsoft Office Excel 2010 spreadsheet program. At this time, it was noticed that not all participants had responded to every question, so the number of participants and that of respondents were different for some items.
Measurements
To measure the degree of agreement with sexual behaviors students answered a 30-item block of the questionnaire in terms of whether they agree or disagree with those. Upon compiling the items, we reviewed the relevant literature, particularly the Hungarian adaptation of the Brief Sexual Attitudes Scale [24] which included 23 items of which we transferred nine items, for example, “It is not necessary for me to become committed with somebody to have sex with her/him”, and “Casual sex is acceptable”. Each item was asked as follows: "Do you agree with the following statements?" The dichotomous responses offered were coded as follows: “I disagree” (0) and “I agree” (1) (Table 1). After having obtained the degree of agreement with each sexual item we calculated the percentage of those participants who agreed with each item then a score was created for each item by dividing the number of agreeing respondents by the total number of respondents.
| Table 1: Questionnaire block for assessing sexual attitudes. | ||
| Do you agree with the following statements? | I agree | I disagree |
| I am happy to initiate having sex with my partner | ||
| The girls must take responsibility for contraception | ||
| The boys must take responsibility for contraception | ||
| It is possible to enjoy sex with someone we do not like particularly | ||
| I consider myself to be full of sexual inhibitions | ||
| I would like to have sex with many partners | ||
| It is okay for girls and boys, to play sex games or self-gratifying sex with each other, even at parties | ||
| Feeling romantic love for my partner is a crucial condition for having sex | ||
| It has already happened that I felt disappointed in having sex | ||
| It is okay if somebody maintains a sexual relationship with several partners at the same time | ||
| I am versed in female sexual anatomy and response | ||
| Oral sex is acceptable | ||
| I am well versed in male sexual anatomy and response | ||
| Casual sex is acceptable | ||
| Anal sex is acceptable | ||
| The idea of sexual violence causes me arousal | ||
| If both partners agree with this, it is okay to have sex as a mutual favor | ||
| Having sex has a culture which can be acquired, and the sex can be learned | ||
| Using sexual aids is acceptable | ||
| Self-gratifying sex is acceptable | ||
| Boys need and enjoy having sex more than girls | ||
| It is not necessary for me to become committed to somebody to have sex with her/him | ||
| I would like to have sex with more than one partner at the same time | ||
| Sex is a very important part of life | ||
| I would like my partner to more often initiate sex | ||
| It has happened that I felt guilty after sex | ||
| Sex is not enjoyable without watching porn pictures or movies | ||
| I would be happy to try sadomasochism with my partner | ||
| It happens that I feel anxious before having sex | ||
| I am happy to have an honest conversation with my partner about sex | ||
Measurement of sexual experience was performed by using a question as follows: "Have you ever had sexual intercourse?" (Have you ever slept with a boy or a girl?)''. The responses offered were as follows: "Yes, I have had sex with 1 female so far", "Yes, I have had sex with several females so far", "Yes, I have had sex with 1 male so far", "Yes, I have had sex with several males so far", "Yes, I have had sex with a female as well as a male so far", and "No". These questions were transferred from the HBSC study [25].
Duration of the current relationship with a partner was measured by the responses to the question as follows: "Are you currently in a relationship with a partner?" The following options were available for responding: "No, I'm single", "Yes, for a few weeks", "Yes, for a few months", "Yes, for more than half a year", "Yes, for more than a year".
The extent of peer relationships was measured by responses to two questions as follows: "How many close male friends do you currently have?" and "How many close female friends do you currently have?" by offering the following response options: "None", "One", "Two, "Three or more". On the other hand, "How often are you meeting your friends outside of school hours before 8 p. m.?" and "How often are you meeting your friends outside of school hours after 8 p. m.?" Responses to these questions were offered as follows: "Rarely or never", "Less than weekly", "Weekly", and "Daily". These questions were transferred from the HBSC study [26].
Statistical analysis
Data were analyzed and encoded using the IBM SPSS version 23. Descriptive statistics, a two-sample t-test, and Spearman rank correlation coefficient were used, and a p - value < 0.05 was considered significant.
Ethics approval
The study was conducted after having received permission from the study site’s institutional ethics review boards. Students signed informed consent to complete the questionnaire. The authors declare that all procedures performed in this study involving participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Demographics
The age of 195 students who responded to the questionnaire ranged from 18 to 22 years (average 19.0 +/- 0.82 years). There was no significant difference in the ages of males and females. Demographic data are summarized in Table 2. Most students' parents completed high school or higher education. Students' mean school marks were typically between 3.5 and 5. The good academic achievement predicted that most of them planned to enter higher education.
| Table 2: Demographics. | ||||
| Students’ number | Percentage | |||
| Gender* | Number of cases | 195 | ||
| Female | 157 | 80.5 | ||
| Male | 38 | 19.5 | ||
| Mean school marks | Range of the mean school grades | |||
| In recent semester | 1 to 2.5 | 2 | 1.02 | |
| 2.6 to 3.4 | 25 | 12.82 | ||
| 3.5 to 4.3 | 67 | 34.35 | ||
| 4.4 to 5.0 | 86 | 44.10 | ||
| In all semesters | 5 | 15 | 7.69 | |
| Out-of-school employment | 43 | 22.1 | ||
| Parents’ highest education level | Mother | Number of cases | 194▲ | |
| Primary school | 5 | 2.58 | ||
| Vocational school | 26 | 13.40 | ||
| High school | 54 | 27.83 | ||
| Tertiary school | 101 | 52.06 | ||
| Other education | 8 | 4.12 | ||
| Father | Number of cases | 193▼ | ||
| Primary school | 7 | 3.62 | ||
| Vocational school | 47 | 24.35 | ||
| High school | 47 | 24.35 | ||
| Tertiary school | 81 | 41.96 | ||
| Other education | 11 | 5.69 | ||
| x Participants՚ mean age was 19.0 +/- 0.82 years, and there was no difference in the age of males and females (p > 0.05). 1,2 Notes: The mother’s education was not given by 1one and the father’s education by 2two participants. |
||||
Features of sexual intercourse with a partner
Of 192 respondents, 67.9% reported having had a sexual relationship. Of the sexually active males, 26.3% had sex with one female, 31.6% with several females, 2.6% with both female and male, 2.6% with one male, 2.6% with several males, and 34.2% had no relationship. Of the sexually active females, 31.6% had sex with one male, 31.6% with several males, 1.9% with one female, 3.2% with both a male and a female, and 31.6% had no sexual relationship. These data demonstrated that approximately one-third of sexually active males and females had more than one sexual partner.
Degree of agreement with oral sex
Of 195 participants, 151 agreed that oral sex was acceptable (77.4%), and 22 did not respond to this question (11.3%). Of 34 male respondents 33 (97.1%), and of 139 female respondents 118 (84.9%) agreed that oral sex was acceptable (p = 0.005). So, altogether the extent of agreement with oral sex amounted to 87.3%. Of 130 respondents who had had sex 115 (88.5%), and of 62 respondents who had not had sex 36 (58.1%) agreed with oral sex. It is of note that among those who had no sexual relationship, the rate of non-respondents was higher (20.9%) compared to those who had sexual experience (4.8%). A score of the agreement with oral sex was found to be 0.9274+/-0.2594 for respondents who had vaginal intercourse, and 0.7347+/-0.4425 for those without sexual experience (p = 0.0061). These data show that prior sexual intercourse increased the degree of agreement with oral sex and the males more agree with oral sex than the females and point out that the students who engaged in vaginal sex also engaged in oral sex.
Participants' relationships with close friends
The number of participants' close friends is summarized in Figure 1. Participants reported that out of males 63.2% had three or more, 23.7% had two, 7.9% had only one, and 5.3% had no close friends, furthermore, out of females 49.7% had three or more, 24.2% had two close friends, 16.6% had only one and 9.6% had no friends. The frequency of meeting close friends outside of school is summarized in Table 3 which indicates that the participants most often met their friends weekly, the females before 8 p.m. and the males after 8 p.m. did it, furthermore, the daily meeting was more common for males than for females. These data demonstrate that students maintained intensive contact with their friends.
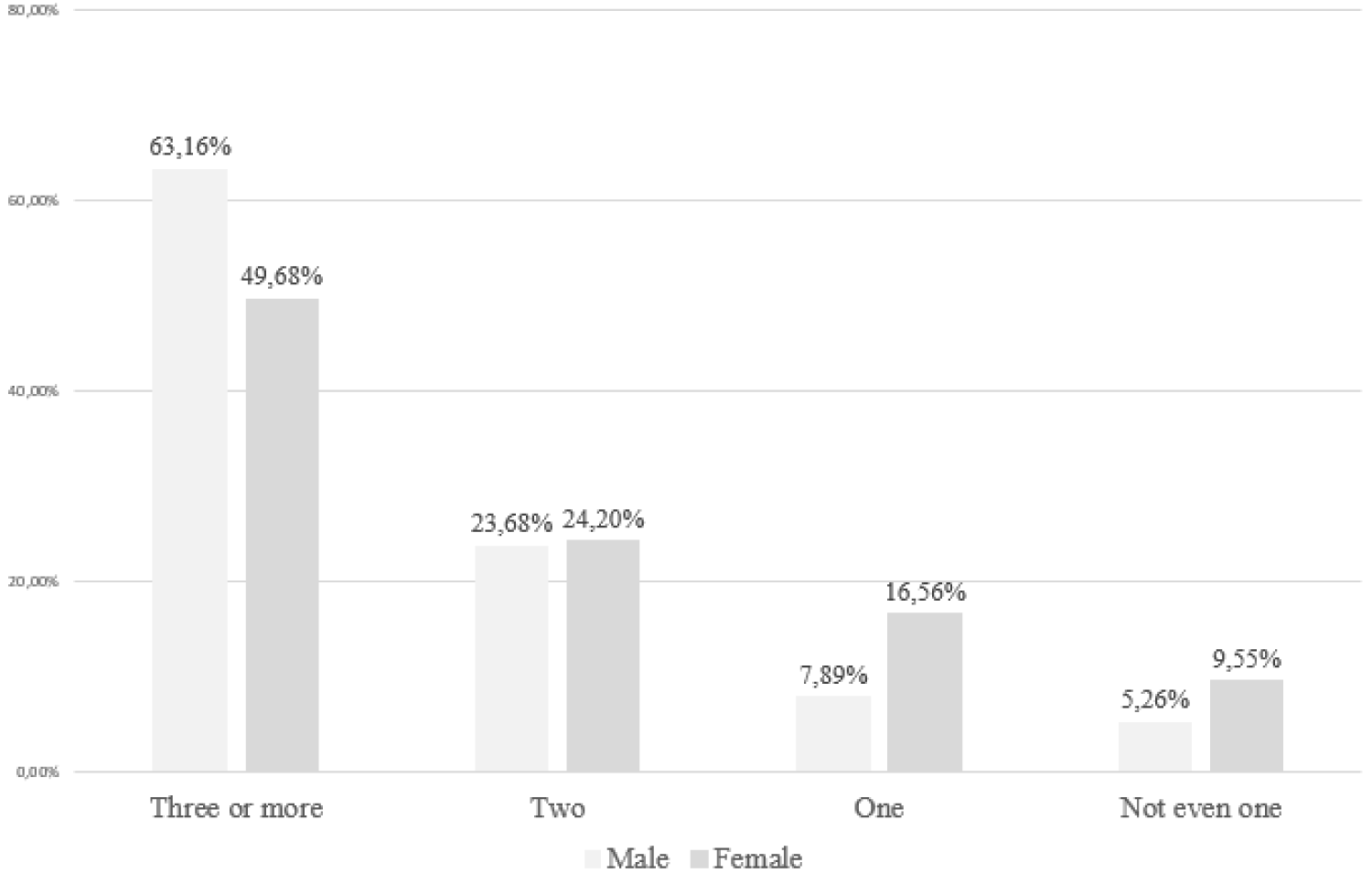
Figure 1: Frequency of number of male and female participants' close friends.
| Table 3: Frequency of meeting close friends outside of school. | ||||||
| Time of meeting | Frequency of meeting | Responder’s number | ||||
| Rarely or never | Less often than weekly | Every week | Every day | |||
| Females (%) | Before 8 p. m. | 10.97 | 28.39 | 47.74 | 12.90 | 155 |
| After 8 p. m. | 9.35 | 5.48 | 38.71 | 7.1 | 156 | |
| Males (%) | Before 8 p. m. | 10.53 | 23.68 | 37.47 | 26.32 | 38 |
| After 8 p. m. | 10.53 | 28.93 | 44.74 | 15.79 | 38 | |
Upon applying Spearman's test, the frequency of meeting friends out-of-school before 8 p.m. (r = 0.238, p = 0.005, n = 138), as well as the frequency of meeting friends out-of-school after 8 p.m. showed a positive correlation with the degree of agreement with oral sex (r = 0.257, p = 0.002, n = 139) for females, but no such correlation was found for males. These data show that the more frequently the females meet their friends, the greater they agree with oral sex.
Duration of current relationship with a partner
Figure 2 illustrates the durations of current relationships with a partner for 192 male and female respondents. 97 (14 males and 83 females) had (50.5%), and 95 (24 males and 71 females) had no current relationship with a partner (49.5%). Ninety students had been in a current partner relationship for at least a few months (46.9%), and 102 had either no current partner relationship or had it only for a few weeks (53.1%). Of the respondents, 12% reported on a current partner relationship lasting for more than six months, and 25.5% reported on that lasting for over one year. These data indicate that the duration of a relationship with a partner is typically short. Upon using the Spearman correlation test, no significant correlation was shown between the degree of agreement with oral sex and the duration of the current relationship with a partner, for neither males (r = 0.133, p >0.05, n = 34) nor females (r = 0.020, p > 0.05, n = 139).
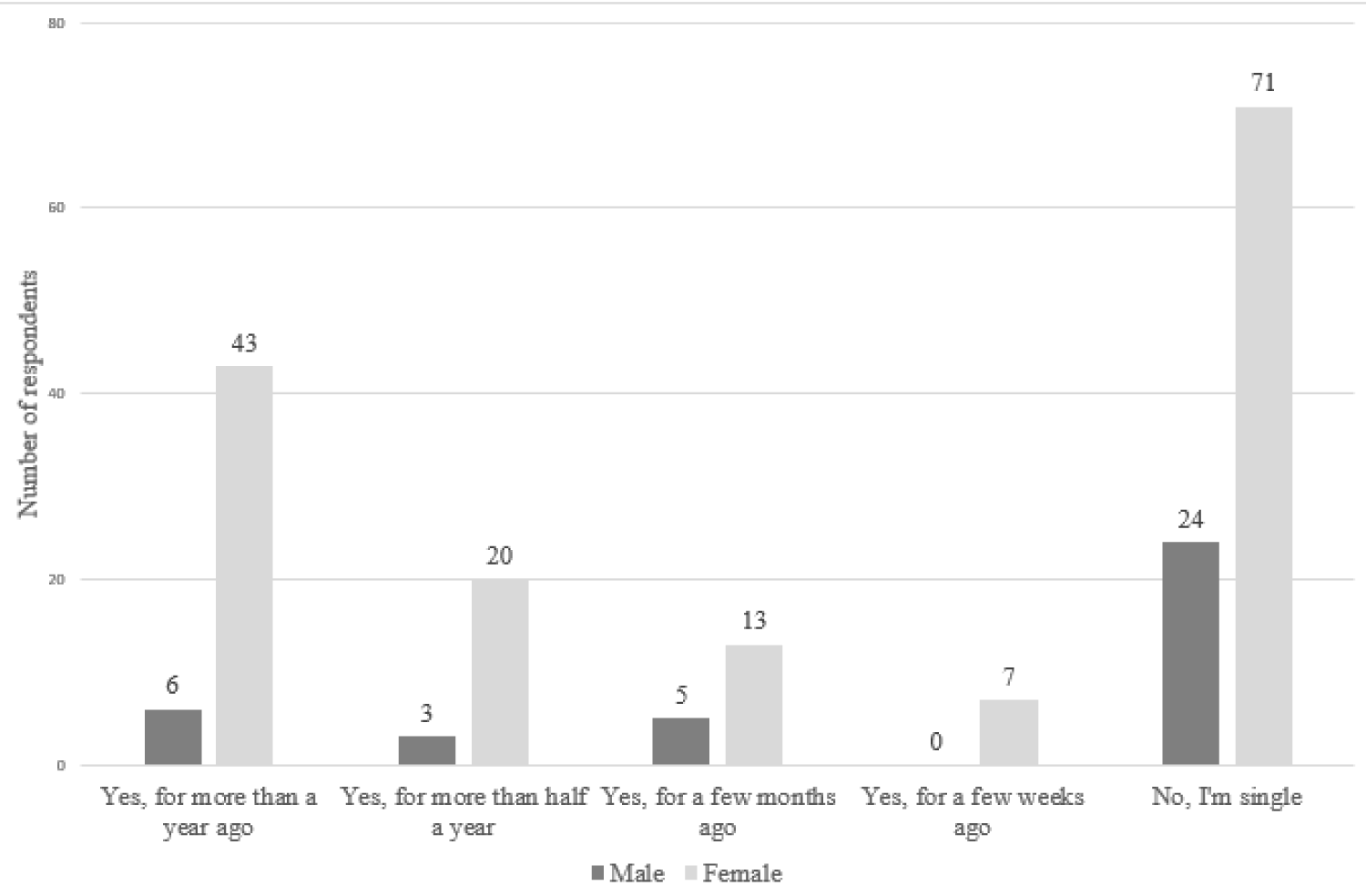
Figure 2: Incidence of the duration of the current relationship with a partner for male and female respondents, expressed in numbers.
Correlations between the agreement with oral sex and agreement with other elements of sexuality
Table 4 summarizes the correlations between the degree of agreement with different items of sexuality presented in Table 1 and the degree of agreement with oral sex. Eighteen out of 30 components of sexuality were found to show some correlation with oral sex. However, it is of note that these correlations show two-way associations. The strongest five correlations which were numbered 1 to 5 may be interpreted as follows: the higher the degree of agreement with self-gratifying sex was, the greater they agreed with oral sex; the higher the degree of agreement with using sexual aids was, the greater they agreed with oral sex; the happier they were to have an honest conversation with their partner about sex, the greater they agreed with oral sex; the happier they were to initiate sex with their partner, the greater they agreed with oral sex; and the more they were well versed in the male sexual anatomy and response, the greater they agreed with oral sex. These data demonstrate that the degree of agreeing with oral sex is associated with the items of sexuality most strongly expressing sexual drive and the desire to gratify it with a partner and is positively linked to the degree of being well-versed in male sexual anatomy and response.
| Table 4: Correlations between the degree of agreement with items of sexuality and the degree of agreement with oral sex. | |||
| Items of sexuality | Spearman correlation | ||
| r | p | n | |
|
0.416 | 0.000 | 172 |
|
0.396 | 0.000 | 167 |
|
0.370 | 0.000 | 164 |
|
0.339 | 0.000 | 170 |
|
0.326 | 0.000 | 173 |
|
0.290 | 0.000 | 170 |
|
0.281 | 0.000 | 171 |
|
0.280 | 0.000 | 173 |
|
0.263 | 0.000 | 173 |
|
0.260 | 0.001 | 172 |
|
-0.199 | 0.009 | 169 |
|
0.196 | 0.010 | 174 |
|
0.187 | 0.016 | 172 |
|
-0.184 | 0.016 | 171 |
|
0.182 | 0.018 | 163 |
|
0.180 | 0.013 | 170 |
|
0.174 | 0.023 | 170 |
|
0.171 | 0.024 | 174 |
| Abbreviations: r = correlation coefficient; p = p - value; n = number of respondents. | |||
The weaker correlations in Table 3 numbered from 6 to 10 show that the degree of accepting oral sex is associated with the degree of agreement with casual sex and anal sex, with accepting the importance of having sex, with accepting being well-versed in female sexual anatomy and response, and with agreeing with that the sexual culture is acquirable. These data suggest that sexual openness also enhances the acceptance of oral sex.
Finally, the degree of agreeing with oral sex was shown to have some additional weak associations marked with numbers 11 to 18 in Table 3. Among these, there were two negative correlations, too, the interpretation of which may be that the more they agreed that the sex is not enjoyable without watching porn, the less they agreed with oral sex; and the more the participants agreed with feeling romantic love for their partner, the less they agreed with accepting oral sex. These data suggest that the rate of agreeing with oral sex may be decreased by both watching porno and feeling romantic love for a partner.
Present findings have revealed that 97.1% of adult high school males and 84.9% of females view oral sex as acceptable. More than half of 15- to 24-year-olds engage in oral sex with a partner of the opposite sex in the U.S. [27], and college students receive oral sex in 79.4% and provide it in 78.4% [20]. In the U.K. 56% of 16- to 18-year-olds had experience with fellatio, and 70% of adolescents who had vaginal intercourse had previously engaged in oral sex [6]. Research has shown that the prevalence of using condoms among young people who have oral sex with opposite-sex partners was 8% to 9%, and young people who have never had sex were less likely to use a condom for oral sex [27]. If considering that the rate of condom use in Hungary generally is low among adolescents [10] and that most students agree with oral sex exactly just because they don’t want to use condoms not to reduce pleasure [6], high acceptance of oral sex predicts both the growing risk for oropharyngeal cancer [28] and the higher risk for preterm birth [16].
Beyond the motivations mentioned at the introduction,
the high prevalence of oral sex may even be attributed to that body scents secreted by sweat and external genitalia (pheromones) reach that sexual partner’s olfactory epithelium in higher concentrations who performs the oral sex, so pheromones can enhance sexual arousal [29,30]. This may explain our finding that those students who reported having had partnered sex, more often agreed with oral sex (88.5%) than those who never had vaginal sex (58.1%).
The present study has also shown that the degree of acceptance of oral sex was positively associated with the degree of agreement with self-gratifying sex and with using sexual aids. These correlations point to the desire to gratify sexual instinct. In addition, the degree of agreement with oral sex was positively correlated with the degree of agreement with the statements that “I am happy to have an honest conversation with my partner about sex, and I am happy to initiate sex with my partner”. These associations suggest that students would like to gratify their sexual instinct with a partner.
The present study has demonstrated a positive correlation between the degree of agreement with being well-versed in male sexual anatomy and response, and the degree of accepting oral sex, which may suggest that females who make up four-fifths of the participants are ready for having oral sex. Furthermore, it was also found for females that the frequency of out-of-school meeting friends was positively associated with the degree of agreement with oral sex. This suggests that sexual information obtained from friends, learning about friends' sexual attitudes and behaviors, and complying with the pressure from friends all contribute to a greater acceptance of oral sex for females. These findings are consistent with the trend that number of the women’s male oral sex partners has increased over the past decade [23].
According to this study, the duration of students' current relationship with a partner was not correlated with the degree of accepting oral sex. In total, only 37.5% of participants reported a current relationship lasting for more than six months. This suggests that most high school students have a short relationship with a partner that favors the growing number of sexual partners.
The current study has shown that 67.9% of respondents reported having had sexual contact and 31.6% of them had more than one sexual partner, and 87.3% of the respondents agreed with oral sex. These findings together suggest a growing number of oral sexual partners. As the high school students and the lay public believe that oral sex has low or no risk [21], the high frequency of accepting oral sexual behavior and the growing number of sexual partners expectedly increase the risk of oral and pharyngeal squamous cell carcinoma caused by HPV infection [28]. At the same time, approximately 10% of HPV infections transmitted by oral or vaginal sex may become permanent, thereby also increasing the risk of uterine cervical cancer [31].
Previously it has been hypothesized that high acceptance of oral sex among youth might be related to low knowledge about the risks of oral sex [8]. The high degree of agreement with oral sex in the current study likely mirrors the insufficient sex education because students recently reported in Hungarian research that sex education at school was not satisfactory [32]. This is consistent with the research that most university students did not know about linking oral sex with oral cancer [19] and that most high school students knew little about spreading HPV [18]. So, we have concluded that poor knowledge about the risks of oral sex also contributes to the high level of agreement with oral sex among youth.
Anyhow, oral sex alone or in combination with vaginal intercourse increases the risk of developing bacterial vaginosis [33], especially if the partner suffers from periodontal disease, even without complaint. Periodontal disease is one of the most common chronic inflammations which may occur even at a young age and is associated with the accumulation of anaerobic bacteria in the oral microbiome. Both the growing number of women's sexual partners prior to pregnancy [34] and men's previous risky sexual behaviors enhance the risk of preterm birth through bacterial vaginosis [35] as well as the risk of oro-pharyngeal and anogenital cancer caused by HPV at a young age [36].
Severe acute complications of the oral sex may occur due to faulty technical execution of it. We are aware of these from medical case reports. A rare risk of oro-genital sex may be the "non-surgical pneumo-peritoneum". This pathology can occur when the partner has blown air into the vagina, which passes on the uterus and enters the abdominal cavity. This condition is associated with abdominal pain and therefore diagnostic surgery is often performed [37]. An additional rare risk of oral sex may be the fatal air embolism caused by blowing air into the vagina [38].
To reduce the health risks of oral sex including the long-term complications such as bacterial vaginosis, preterm birth, genital as well as oropharyngeal cancers, and short-term complications such as pneumoperitoneum and air embolism, we recommend that high schools put aside taboos and provide students exact and scientific knowledge not only about the potential complications of vaginal sex but also about the consequences of oral sex, thereby raising awareness since many adolescents begin sexual contact even during the high school years.
Summary
Agreement with oral sex is high among high school students. The degree of agreeing with oral sex is enhanced for females, by an intensive relationship with close friends, furthermore, by the previous sexual relationship and the agreement with those items of sexuality that express a high sexual drive and its wantedness to gratify it with a partner, and by the greater agreement with some dimensions expressing sexual openness.
Limitations of the study
Limitations of this study include the self-reports on sexual experience, which is sensitive data, the low proportion of men in the sample due to differences in attitudes between men and women, and missing responses to some questions resulting from the fact that all participants didn’t respond each question, furthermore, that the oral sex was not divided into provider and receiver. Future studies with higher numbers are needed to confirm the explored associations within sexual attitudes.
Considering that the acceptance of oral sex is high among high school students, the rate of sexually active students is high, many of them also have already had more than one sexual partner, and they don’t always use a condom, moreover, they might choose oral sex just because to want to avoid using a condom for the sake of greater pleasure, accepting oral sex has some risks for them. Therefore, we recommend continuing the sex education programs in high school and focusing on the risks of oral sex.
The authors are grateful to Klára Soltész-Várhelyi (Pázmány Péter Catholic University, Faculty of Humanities and Social Sciences, Budapest) for assistance in the statistical analysis of the present study.
Author's division of labor
M. Z.: Editing the questionnaire, conducting the study, evaluating the results, and compiling the manuscript. A. P: Evaluation of the results, review of the literature, compilation of the manuscript. K. Z.: Conducting research, and processing data. T. H. P.: Checking the manuscript, casting it into the final form.
- Blake DKP, Knox D, Zusman ME. Exploring social sexual scripts related to oral sex: A profile of college student perceptions. Prof Couns. 2012; 2:1-11. http://tpcjournal.nbcc.org doi:10.15241/kpd.2.1.1
- Cornell JL, Halpern-Felsher BL. Adolescents tell us why teens have oral sex. J Adolesc Health. 2006 Mar;38(3):299-301. doi: 10.1016/j.jadohealth.2005.04.015. PMID: 16488832.
- Goldstein R, Halpern-Felsher B. Adolescent Oral Sex and Condom Use: How Much Should We Worry and What Can We Do? J Adolesc Health. 2018 Apr;62(4):363-364. doi: 10.1016/j.jadohealth.2018.01.002. PMID: 29571434.
- Pakpahan C, Darmadi D, Agustinus A, Rezano A. Framing and understanding the whole aspect of oral sex from social and health perspectives: a narrative review. F1000Res. 2022 Feb 14; 11:177. doi: 10.12688/f1000research.108675.3. PMID: 36035886; PMCID: PMC9377381.
- Richters J, Visser Rd, Rissel C, Smith A. Sexual practices at last heterosexual encounter and occurrence of orgasm in a national survey. J Sex Res. 2006 Aug;43(3):217-26. doi: 10.1080/00224490609552320. PMID: 17599244.
- Stone N, Hatherall B, Ingham R, McEachran J. Oral sex and condom use among young people in the United Kingdom. Perspect Sex Reprod Health. 2006 Mar;38(1):6-12. doi: 10.1363/psrh.38.006.06. PMID: 16554266.
- Habel MA, Leichliter JS, Dittus PJ, Spicknall IH, Aral SO. Heterosexual Anal and Oral Sex in Adolescents and Adults in the United States, 2011-2015. Sex Transm Dis. 2018 Dec;45(12):775-782. doi: 10.1097/OLQ.0000000000000889. PMID: 29965947; PMCID: PMC6753934.
- Santa-Bárbara RC, Hueso-Montoro C, Martín-Salvador A, Álvarez-Serrano MA, Gázquez-López M, Pérez-Morente MÁ. Association between Sexual Habits and Sexually Transmitted Infections at a Specialised Centre in Granada (Spain). Int J Environ Res Public Health. 2020 Sep 21;17(18):6881. doi: 10.3390/ijerph17186881. PMID: 32967101; PMCID: PMC7557876.
- Health Behavior in School-aged Children (HBSC) Survey. HBSC 2017/18 Open Access data file documentation 2017/18 (ed. 1.0). 2022; 69-70. https://hbsc.org/publications/reports/
- Gyarmathy VA, Thomas RP, Mikl J, McNutt LA, Morse DL, DeHovitz J, Ujhelyi E, Számadó S. Sexual activity and condom use among Eastern European adolescents--the Study of Hungarian Adolescent Risk Behaviours. Int J STD AIDS. 2002 Jun;13(6):399-405. doi: 10.1258/095646202760029822. PMID: 12015014; PMCID: PMC5666688.
- Galamb A, Pajor A, Langmár Z, Sobel G. Results of the first human papilloma virus center in Hungary (2007-2011). Orv Hetil. 2011 Nov 6;152(45):1804-7. Hungarian. doi: 10.1556/OH.2011.29233. PMID: 22011366.
- Brown B, Blas MM, Cabral A, Carcamo C, Gravitt PE, Halsey N. Oral sex practices, oral human papillomavirus and correlations between oral and cervical human papillomavirus prevalence among female sex workers in Lima, Peru. Int J STD AIDS. 2011 Nov;22(11):655-8. doi: 10.1258/ijsa.2011.010541. PMID: 22096051; PMCID: PMC4699621.
- Agarwal K, Robinson LS, Aggarwal S, Foster LR, Hernandez-Leyva A, Lin H, Tortelli BA, O'Brien VP, Miller L, Kau AL, Reno H, Gilbert NM, Lewis WG, Lewis AL. Glycan cross-feeding supports mutualism between Fusobacterium and the vaginal microbiota. PLoS Biol. 2020 Aug 25;18(8):e3000788. doi: 10.1371/journal.pbio.3000788. PMID: 32841232; PMCID: PMC7447053.
- Chen X, Lu Y, Chen T, Li R. The Female Vaginal Microbiome in Health and Bacterial Vaginosis. Front Cell Infect Microbiol. 2021 Apr 7; 11:631972. doi: 10.3389/fcimb.2021.631972. PMID: 33898328; PMCID: PMC8058480.
- Chu DM, Seferovic M, Pace RM, Aagaard KM. The microbiome in preterm birth. Best Pract Res Clin Obstet Gynaecol. 2018 Oct; 52:103-113. doi: 10.1016/j.bpobgyn.2018.03.006. Epub 2018 Apr 9. PMID: 29753695.
- Wiik J, Nilsson S, Kärrberg C, Strander B, Jacobsson B, Sengpiel V. Associations of treated and untreated human papillomavirus infection with preterm delivery and neonatal mortality: A Swedish population-based study. PLoS Med. 2021 May 10;18(5):e1003641. doi: 10.1371/journal.pmed.1003641. PMID: 33970907; PMCID: PMC8143418.
- EMMI (Ministry of Human Resources): Health professional guidelines for the diagnosis, prevention, and treatment of imminent preterm birth. Professional Guideline 2020. https://www.hbcs.hu/uploads/jogszabaly/3272/fajlok/2020_EuK_19_szam_EMMI_szakmai_iranyelv_4.pdf
- Varga-Tóth A, Németh G, Paulik E. Medical aspects of sexual education according to national and international guidelines. Orv Hetil. 2019 Mar;160(13):494-501. Hungarian. doi: 10.1556/650.2019.31359. PMID: 30907103.
- Lewandowski B, Czenczek-Lewandowska E, Pakla P, Frańczak J, Piskadło T, Migut M, Brodowski R. Awareness of Polish undergraduate and graduate students regarding the impact of viral infections and high-risk sexual behaviors on the occurrence of oral cancer. Medicine (Baltimore). 2018 Oct;97(41):e12846. doi: 10.1097/MD.0000000000012846. PMID: 30313122; PMCID: PMC6203533.
- Herbenick D, Patterson C, Beckmeyer J, Gonzalez YRR, Luetke M, Guerra-Reyes L, Eastman-Mueller H, Valdivia DS, Rosenberg M. Diverse Sexual Behaviors in Undergraduate Students: Findings from a Campus Probability Survey. J Sex Med. 2021 Jun;18(6):1024-1041. doi: 10.1016/j.jsxm.2021.03.006. Epub 2021 May 19. PMID: 34020921.
- Brondani MA, Siqueira AB, Alves CMC. Exploring lay public and dental professional knowledge around HPV transmission via oral sex and oral cancer development. BMC Public Health. 2019 Nov 15;19(1):1529. doi: 10.1186/s12889-019-7923-6. PMID: 31729969; PMCID: PMC6858745.
- da Cunha AR, Bessel M, Hugo FN, de Souza FMA, Pereira GFM, Wendland EMDR. Sexual behavior and its association with persistent oral lesions: analysis of the POP-Brazil study. Clin Oral Investig. 2021 Mar;25(3):1107-1116. doi: 10.1007/s00784-020-03407-0. Epub 2020 Jun 25. PMID: 32583241; PMCID: PMC7878220.
- Katz DA, Copen CE, Haderxhanaj LT, Hogben M, Goodreau SM, Spicknall IH, Hamilton DT. Changes in Oral and Anal Sex with Opposite-Sex Partners Among Sexually Active Females and Males Aged 15 to 44 Years in the United States: National Survey of Family Growth, 2011-2019. Sex Transm Dis. 2023 Nov 1;50(11):713-719. doi: 10.1097/OLQ.0000000000001867. Epub 2023 Sep 11. PMID: 37732840; PMCID: PMC10581427.
- Csonka B, Szabó M, Szabó Á, Hevesi K. Hungarian adaptation of the Brief Sexual Attitudes Scale (BSAS). Alk Pszich. 2017; 17:101-113. [Hungarian] https://doi.org/10.17627/ALKPSZICH.2017.1.101
- Költő A. Sexual behavior and romantic experiences. In Health Behaviour in School-aged Children (HBSC): A WHO-collaborative Cross-National Study, National Report. 2014; 121-130. Németh Á, Költő A (eds). [Hungarian] https://mek.oszk.hu/16100/16119/16119.pdf
- Zsíros E, Németh Á, Költő A. Peer relationships. In Health Behaviour in School-aged Children (HBSC): A WHO-collaborative Cross-National Study, National Report. 2014; 109-120. (eds). [Hungarian] https://mek.oszk.hu/16100/16119/16119.pdf
- Holway GV, Hernandez SM. Oral Sex and Condom Use in a U.S. National Sample of Adolescents and Young Adults. J Adolesc Health. 2018 Apr;62(4):402-410. doi: 10.1016/j.jadohealth.2017.08.022. Epub 2017 Nov 22. PMID: 29174873.
- Fernández-López C, Morales-Angulo C. Otorhinolaryngology manifestations secondary to oral sex. Acta Otorrinolaringol Esp (Engl Ed). 2017 May-Jun;68(3):169-180. English, Spanish. doi: 10.1016/j.otorri.2016.04.003. Epub 2016 Oct 25. PMID: 27793330.
- Oren C, Peled-Avron L, Shamay-Tsoory SG. A scent of romance: human putative pheromone affects men's sexual cognition. Soc Cogn Affect Neurosci. 2019 Jul 31;14(7):719-726. doi: 10.1093/scan/nsz051. PMID: 31309986; PMCID: PMC6778825.
- Ye Y, Lu Z, Zhou W. Pheromone effects on the human hypothalamus in relation to sexual orientation and gender. Handb Clin Neurol. 2021; 182:293-306. doi: 10.1016/B978-0-12-819973-2.00021-6. PMID: 34266600.
- Cervical cancer - World Health Organization (WHO). https://www.who.int/news-room/fact-heets/detail/cervical-cancer. Hungarian. 2022.
- Semsey G. Practice of the sexual education in Hungarian high schools. Thesis of PhD dissertation. 2016. https://edit.elte.hu/xmlui/bitstream/handle/10831/37709/Semsey_G%C3%A1bor_t%C3%A9zisf%C3%BCzet_magyar.pdf
- Koumans EH, Sternberg M, Bruce C, McQuillan G, Kendrick J, Sutton M, Markowitz LE. The prevalence of bacterial vaginosis in the United States, 2001-2004; associations with symptoms, sexual behaviors, and reproductive health. Sex Transm Dis. 2007 Nov;34(11):864-9. doi: 10.1097/OLQ.0b013e318074e565. PMID: 17621244.
- Yost NP, Owen J, Berghella V, Thom E, Swain M, Dildy GA 3rd, Miodovnik M, Langer O, Sibai B; National Institute of Child Health and Human Development, Maternal-Fetal Medicine Units Network. Effect of coitus on recurrent preterm birth. Obstet Gynecol. 2006 Apr;107(4):793-7. doi: 10.1097/01.AOG.0000206757.92602.b5. PMID: 16582114.
- Paul K, Garcia PJ, Manhart LE, Holmes KK, Hitti JE. Partner- and partnership-related risk factors for preterm birth among low-income women in Lima, Peru. Soc Sci Med. 2009 Apr;68(8):1535-40. doi: 10.1016/j.socscimed.2009.02.027. Epub 2009 Mar 11. PMID: 19282077.
- Nguyen NP, Nguyen LM, Thomas S. Oral sex and oropharyngeal cancer. Medicine (Baltimore). 2000; 95:1936-1959. doi: 10.1097/md.00000000000042
- Cawich SO, Johnson PB, Williams E, Naraynsingh V. Non-surgical pneumoperitoneum after oro-genital intercourse. Int J Surg Case Rep. 2013;4(11):1048-51. doi: 10.1016/j.ijscr.2013.08.022. Epub 2013 Sep 25. PMID: 24121052; PMCID: PMC3825970.
- Truhlar A, Cerny V, Dostal P, Solar M, Parizkova R, Hruba I, Zabka L. Out-of-hospital cardiac arrest from air embolism during sexual intercourse: case report and review of the literature. Resuscitation. 2007 Jun;73(3):475-84. doi: 10.1016/j.resuscitation.2006.10.004. Epub 2007 Feb 8. PMID: 17291667.