
More Information
Submitted: May 24, 2021 | Approved: June 10, 2021 | Published: June 11, 2021
How to cite this article: Shiddo D, Nour N. Factors associated with Female Genital Mutilation among daughters of reproductive aged women at Academic Charity Teaching Hospital (ACTH). Clin J Obstet Gynecol. 2021; 4: 073-080.
DOI: 10.29328/journal.cjog.1001092
Copyright License: © 2021 Shiddo D, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abbreviations: ACTH: Academic Charity Teaching Hospital; FGM: Female Genital Mutilation

Factors associated with Female Genital Mutilation among daughters of reproductive aged women at Academic Charity Teaching Hospital (ACTH)
Danyah Shiddo1* and Hilmi Nour2
1Department of Research Methodology & Biostatistics, Faculty of Medicine, University of Medical Sciences & Technology, Khartoum, Sudan
2Senior Consultant, Obstetrics and Gynecology, Academic Charity Teaching Hospital, Khartoum, Sudan
*Address for Correspondence: Dr. Danyah Shiddo, Department of Research Methodology & Biostatistics, Faculty of Medicine, University of Medical Sciences & Technology, Khartoum, Sudan, Email: [email protected]
Introduction: It is estimated that more than 200 million girls and women alive today have undergone female genital mutilation. Female genital mutilation still remains to be a serious problem for large proportion of women in most sub-Saharan Africa countries including Sudan, with a high prevalence of 88%.
Objective: The main objective was to identify the factors associated with FGM among daughters of reproductive aged woman.
Materials and methods: A community based cross-sectional study was conducted on 200 mothers, the total sample was collected in ACTH based on the number of reproductive age mothers with at least one daughter older than 5 years. A structured and interviewer administered questionnaire was used to collect data. The data obtained was analyzed by the use of the SPSS software.
Results: Out of 200 mothers, 113 (56.5%) had at least one circumcised daughter. Knowledge about genital mutilation (AOR = 4.29, 95% CI: 1.13-15.37), attitude (AOR = 48.53, 95% CI: 14.45-198.69) and mothers circumcision status (AOR = 14.03, 95% CI: 2.81- 95.45) were the most significantly associated with FGM. Furthermore, having good knowledge, positive attitude, high socio-economic status, being literate, being of Christian religion and living in urban area had lower odds of having a circumcised daughter.
Conclusion: In this study, more than half of the mothers had at least one circumcised daughter. Mothers’ knowledge, attitude, circumcision status, socio-economic status, age, residence, educational level and religion were significantly associated with female genital mutilation.
Female genital mutilation (FGM) comprises all procedures that involve partial or total removal of the external female genitalia, or other injury to the female genital organs for non-medical reasons [2].
The World Health Organization (WHO) has identified four types of FGM:
Type I, also called clitoridectomy: Partial or total removal of the clitoris and/or the prepuce.
Type II, also called excision: Partial or total removal of the clitoris and the labia minora, with or without excision of the labia majora. The amount of tissue that is removed varies widely from community to community.
Type III, also called infibulation: Narrowing of the vaginal orifice with a covering seal. The seal is formed by cutting and re-positioning the labia minora and/or the labia majora. This can take place with or without removal of the clitoris.
Type IV: All other harmful procedures to the female genitalia for non-medical purposes, for example: pricking, piercing, incising, scraping or cauterization [3].
An estimated 200 million girls and women alive today are believed to have been subjected to FGM; but rates of FGM are increasing, a reflection of global population growth. Girls and women who have undergone FGM live predominately in sub-Saharan Africa and the Arab States, but FGM is also practiced in select countries in Asia, Eastern Europe and Latin America. It is also practiced among migrant populations throughout Europe, North America, Australia and New Zealand [3].
In Africa, FGM is known to be practiced among certain communities in 29 countries: Benin, Burkina Faso, Cameroon, Central African Republic, Chad, Cote d'Ivoire, Democratic Republic of Congo, Djibouti, Egypt, Eritrea, Ethiopia, Gambia, Ghana, Guinea, Guinea-Bissau, Kenya, Liberia, Mali, Mauritania, Niger, Nigeria, Senegal, Sierra Leone, Somalia, Sudan, Tanzania, Togo, Uganda and Zambia [3].
As compared to other African countries where incidence has decreased, Sudan is one the few countries that still persists on this practice, with 88% of women aged 15-49 have undergone some form of FGM [4] and an estimated 9 out of 10 Sudanese women aged 15 to 49 have been cut [5].
In Sudan, Type 1 is known as Sunna, and generally entails only removal of the tip of the prepuce. The intermediate Type 2 is referred to as Matwasat, and Type 3 is known as Pharaonic [6]. The most prevalent type of FGM practiced in Sudan is Type III (74%), with 23% having the least severe “Sunna” type (Type I) and 2% an “intermediate” form (Type II) (these figures are for urban areas, the figures for rural areas are 77%, 19% and 1% respectively) [7].
FGM is recognized internationally as a violation of the human rights of girls and women. It reflects deep-rooted inequality between the sexes, and constitutes an extreme form of discrimination against women. It is nearly always carried out on minors and is a violation of the rights of children. The practice also violates a person's rights to health, security and physical integrity, the right to be free from torture and cruel, inhuman or degrading treatment, and the right to life when the procedure results in death [2].
Experience of FGM increases the short and long term health risks to women and girls and is unacceptable from a human rights and health perspective. The health consequences vary according to the type and severity of the procedure performed. Short term complications of FGM include: Severe pain, excessive bleeding, shock, genital tissue swelling, HIV, Urination problems, impaired wound healing and death. The long term complications of FGM Types I, II and III (occurring at any time during life) include: Chronic genital infections, Urinary tract infections, painful urination, menstrual disturbances (Dysmenorrhea, irregular menses and difficulty passing blood), keloids, HIV, sexual problems (pain during intercourse, decreased satisfaction, etc.), obstetric problems (FGM is associated with an increased risk of Caesarean section, post-partum hemorrhage, recourse to episiotomy, difficult labour, obstetric tears/lacerations, instrumental delivery, prolonged labour, and extended maternal hospital stay. The risks increase with the severity of FGM), perinatal risks, psychological consequences (post-traumatic stress disorder, anxiety disorders and depression) [8].
A study conducted by Alia, et al. (2006) in Khartoum, Sudan aimed to estimate the prevalence of FGM, identify the types performed and investigate whether FGM is associated with various social factors. A total of 255 girls aged 4-9 presenting to a pediatric emergency ward were recruited. A detailed history was obtained and full examination, including inspection of the genitalia, was performed to verify the type and extent of FGM. Results revealed that 20% of the study group had undergone FGM, 50% of guardians indicated that it would be done later, and 29% stated that the child would not undergo FGM. Those who had allowed or intended to allow their daughters to undergo FGM were of significantly lower socio-economic status (p = 0.0008) and had spent significantly fewer years in school (both mothers, p = 0.0015, and fathers, p = 0.0266) than those who had not/would not. All who had undergone FGM were Muslims. None of the 16 Christians had undergone FGM. The study concluded that FGM is still practiced widely in Khartoum and probably in many parts of northern Sudan and the type undertaken is often the most severe. Parental education, socio-economic level and religion are important determinants of the practice, but social pressure on parents and girls seems to play an important role [9].
A second study was carried out by Getnet, et al, (2009) with the aim to determine the prevalence and associated factors of FGM among Somali refugees in Eastern Ethiopia, preformed a cross-sectional study on 492 respondents sampled from three refugee camps in Somali Regional State. The results revealed that although the intention of the parents to circumcise their daughters was high (84%), 42.4% of 288 girls aged ≤ 12 were reported being undergone FGM. The prevalence increased with age, and about 52% and 95% were circumcised at the age of 7–8 and 11–12 years, respectively. The study concluded that FGM is widely practiced among the Somali refugee community in Eastern Ethiopia, and there was a considerable support for the continuation of the practice particularly among women. The findings indicate a reported shift of FGM from its severe form to milder clitoral cutting. More men than women positively viewed anti-FGM interventions, and fewer men than women had the intention to let their daughters undergo FGM [10].
A third study conducted by Joseph, et al. (2010) examined whether the prevalence of FGM changed overtime and identified the factors associated with this practice in Burkina Faso. The results revealed that of the 3,289 Burkinabe women (aged 15-49) who participated in the survey, 2,240 (68.1%) underwent FGM. Among women who had a daughter (n = 2,258), 18.7% had a daughter who underwent FGM. Young age [15 to 24 years (odd ratio (OR): 0.26. 95% confidence interval (CI) 0.21 to 0.31) or 25 to 34 years (OR 0.59, 95% CI 0.48 to 0.72)], ethnicity [Gourmatche ethnic group (OR: 0.48, 95% CI 0.31 to 0.73)], religion [Muslim (OR: 1.53, 95% CI 1.09 to 2.14)], and social support from community leaders (OR: 1.37, 95% CI 1.07 to 1.75) were significantly associated with the FGM among women in Burkina Faso. The study concluded that the practice of FGM is still high in Burkina Faso, However, the low prevalence of FGM among younger women and their daughters may be an indication of behavior change [11].
Another study conducted by Tesfaye, et al. (2011) aimed to assess the spatial distribution and factors associated with FGM among reproductive age women in the country. The method used a population based national representative surveys and data from two (2000 and 2005) Ethiopian demographic and health surveys (EDHS) were used in the analysis. A total of 15,367 (from EDHS 2000) and 14,070 (from EDHS 2005) women of reproductive age (15–49 years) were included in the analysis. The results showed that the prevalence has been decreasing. Being wealthy, Muslim and in higher age categories are associated with increased odds of FGM among women. Similarly, daughters from Muslim women have increased odds of experiencing FGM. Women in the higher age categories have increased odds of having daughters who experience FGM. The odds of FGM among daughters decrease with increased maternal education. Mass media exposure, being wealthy and higher paternal and maternal education are associated with decreased odds of women’s support of FGM continuation. The study concluded that individual, economic, socio-demographic, religious and cultural factors played major roles in the existing practice and continuation of FGM [12].
A cross-sectional study conducted by Andualem, (2012) aimed to assess the prevalence and associated factors for female genital cutting in Amhara Region, Ethiopia. A total of 730 mothers participated in the study. Results revealed that the prevalence of FGM was higher, 62.7% on under five daughters in the study area. Health education (AOR = 0.19; 95%, CI = 0.08-0.45), age 15-24 years [AOR (95% CI) = 0.20 (0.06-0.64)], women’s educational status [AOR (95% CI) = 5.43 (1.88, 55.68)], women themselves circumcised [AOR (95% CI) = 3.45 (1.35, 8.79)] and criminal [AOR (95% CI) = 0.37 (0.16, 0.86)] were found significantly associated with FGM. It concluded that;
Female genital cutting was highly practiced among rural women than urban. Age, educational status, residence, being circumcised, health education, knowledge on female denial cutting and believing it as criminal were found to be determinants of female genital cutting [14].
Another cross-sectional study conducted by Mulugeta et al (2014) aimed to determine the prevalence and associated factors of FGM in Hababo Guduru District, Western Ethiopia was conducted on 610 mothers. Results revealed that out of 610 mothers, 293 (48%) had at least one circumcised daughter. Having a good knowledge about genital mutilation (Adjusted Odds Ratio [AOR] = 0. 14, 95% CI: 0.09–0.23), positive attitude (AOR = 0. 26, 95% CI: 0.16–0.43), being literate (AOR = 0.50, CI: 0.28–0.91) and living in urban area (AOR = 0.30, 95% CI: 0.17–0.51) had a lower odds of female genital mutilation. In addition, not knowing genital mutilation as a crime (AOR = 5, 95% CI: 3.07–8.19), and being in the age group of 40–49 (AOR = 2.56, 95% CI: 1.40–4.69) had a higher odds of having circumcised daughter. This study concluded that in this study, about half of the mothers had at least one circumcised daughter. Mothers’ knowledge, attitude, age, residence, educational status and fathers’ religion were significantly associated with female genital mutilation [16].
A study conducted by Desalegn, et al. (2017) aimed to assess prevalence of female genital mutilation (FGM) as well as identifying its associated factors among high school students in Dale Wabera Woreda, Oromia Regional State, Ethiopia using an Institution based cross sectional study design. Data were collected from 769 study participants with a response rate of 96.4%. The overall prevalence of FGM among the study participants was 77.8%; 95% CI (74.9%, 80.7%). Among the age groups, those ≥ 17 years were at higher odds of practicing FGM compared to the other age group [AOR 1.8; 95% CI (1.28, 2.6). The odds of FGM was higher in grades eleven and twelve students compared to grade nine [AOR = 2.98, 95% CI (1.45, 6.12)] and [AOR = 6.52, 95% CI (1.85, 22.94)], respectively. Residence was one of the factors independently associated with magnitude of FGM given that the chance of being mutilated was higher in students from rural area compared to those urban residents [AOR = 1.6, 95% CI (1.01, 2.52)]. The other factor independently associated with FGM was mother occupation. The odds of practicing FGM was higher among female students whose mothers were housewives and merchants compared to those with government employee mothers after adjusting for age, grade, and residence [AOR 2.38; 95% CI (1.07, 5.29)] and [AOR 2.72; 95% CI (1.04, 7.12)], respectively. The study concluded that study participants with age ≥ 17, grades 11 and 12, residing in rural area, and having housewives and merchant mothers’ occupation were at higher odds of FGM [18].
Rationale
Female Genital Mutilation is widely practiced in Sudan. It is a serious threat to women’s health, a violation to human rights that has absolutely no benefit and is associated with many health complications and longer term obstetric, gynaecological, psychosocial and sexual consequences.
Although endless studies about the negative impact and consequences of FGM have been carried out, the cultural practice still persists. Therefore it is crucial to understand and try to address the reasons and factors for its persistence.
General objective
To identify the factors associated with female genital mutilation among daughters of reproductive aged women.
Specific objectives
• To compare the prevalence of FGM among daughters of circumcised and non-circumcised mothers
• To compare the knowledge about ill effects of FGM among the mothers of circumcised and uncircumcised daughters
• To determine the relationship between mothers socio-demographic characteristics and daughters circumcision status
• To determine relationship between daughters circumcision status and mothers socioeconomic status
Study design
Community based cross-sectional analytic study design was employed.
Study population
All reproductive aged women attending the Obstetrics & Gynecology outpatient clinic at ACTH for different complaints during the study period (1st September to 31st December) were recruited to participate in the study, who have at least one daughter greater than 5 years of age.
Study area
This study was conducted in Academic Charity Teaching Hospital, which is a charity teaching hospital that provides service for rural and urban parts of Khartoum state and mainly linked to the University of Medical Sciences and Technology. The obstetric department consists of a labor room, theatre, wards.
The hospital perform roughly 3600 deliveries per year. There are five ante-natal clinics per week, from Sunday to Thursday, covered by five senior consultants.
Sample size and sampling technique
200 women were included in the study between 1st of September and 31st of December. Data was collected by convenient sampling.
Study subject: Selection and definition
• Inclusion criteria: All reproductive aged women attending the Obstetrics and Gynecology outpatient clinic in ACTH in the time period 1/9/2017 to 31/12/2017 who have at least one daughter older than 5 years old.
• Exclusion criteria: Non-Sudanese mothers that attended the clinic and those who did not agree to take part in the study.
Data collection methods and tools
Data was collected via a structured and interviewer administered questionnaire.
Data analysis
Data was analyzed by using Statistical Program for Social Science (SPSS) version 17 and Microsoft Excel. It was be presented in form of tables, pie or bar charts. Chi-square was be used for statistical significance (alpha level = 0.05.)
Variables
• Dependent variable: FGM status of daughter
• Independent variable: Age, Residence, Origin, Educa-tional level, Mothers occupation, Fathers occupation, Religion, Mothers circumcision status, knowledge of ill effects and attitude towards FGM
Limitations
• This study did not assess community related factors such as norms, beliefs and cultural values which influence FGM practice
• Results cannot be generalized as it only showed one hospital in Khartoum
• Few number of Christian women participated in the study
Ethics
It was sought from the Research technical and ethical committee and the Faculty of Medicine, University of Medical Sciences and Technology, Informed consent from the management of Academy Teaching Hospital. Verbal consent from the patients was obtained and their privacy and confidentiality was maintained.
The aim of this study was to identify factors associated with Female Genital Mutilation (Circumcision) among daughters of reproductive aged women. Specifically, we aimed to elucidate the prevalence of women with circumcised daughters. To assess the association between Knowledge of Ill Effects of FGM and Circumcision Status of Daughters. As well as to assess the association between Attitude towards FGM and Daughters’ Circumcision status. Finally we aimed to elucidate which socio-demographic factors were associated with daughters’ circumcision status.
Demographics
A total of 200 participants were included in this study. The majority had at least one daughter circumcised at 113(56.5%). Mean maternal age was 32.4 ± 5.76 with a statistically significant difference between mothers who had at least one daughter circumcised and those that had none. Most mothers, 166(83%) were housewives, with no significant association between Maternal Occupation and FGM. Religion was significantly associated with FGM where 95% were of the sample were of Muslims, with only 2/10(20%) of those who were Christians had FGM. Residence as well as Origin were significantly associated with FGM.
Tests of association
Multiple other factors not shown on table 1 above were tested for Association with FGM using Chi-Squared or Fisher’s Exact Test wherever applicable. Odd ratios and Confidence Intervals were also computed. Show in table 2 and the figures 1-3. All the previous variable were unequivocally associated with FGM with very large OR and safe Confidence Intervals.
| Table 1: Participants Demographics Stratified by Circumcision Status. | ||||
| Overall | At Least One Daughter Circumcised | |||
| No | Yes | p | ||
| n | 200 | 87 (43.5) | 113(56.5) | |
| Maternal Age (mean (sd)) | 32.45 (5.76) | 31.45 (5.40) | 33.21 (5.92) | 0.031 |
| Maternal Occupation (%) | ||||
| Housewife | 166 (83.0) | 68 (78.2) | 98 (86.7) | 0.084 |
| Non-Professional | 25 (12.5) | 12 (13.8) | 13 (11.5) | |
| Professional | 9 (4.5) | 7 (8.0) | 2 (1.8) | |
| Religion (%) | ||||
| Muslim | 190 (95.0) | 79 (90.8) | 111 (98.2) | 0.039 |
| Christian | 10 (5.0) | 8 (9.2) | 2 (1.8) | |
| Residence (%) | ||||
| Urban | 173 (86.5) | 84 (96.6) | 89 (78.8) | 0.001 |
| Rural | 27 (13.5) | 3 (3.4) | 24 (21.2) | |
| Origin (%) | ||||
| North | 16 (8.0) | 8 (9.2) | 8 (7.1) | <0.001 |
| East | 27 (13.5) | 7 (8.0) | 20 (17.7) | |
| West | 52 (26.0) | 16 (18.4) | 36 (31.9) | |
| South | 17 (8.5) | 15 (17.2) | 2 (1.8) | |
| Central | 88 (44.0) | 41 (47.1) | 47 (41.6) | |
| Table 2: Factors Associated FGM. | ||||||
| Daughter Circumcised | Odds Ratio | 95% CI of OR | p - value | |||
| No | Yes | Lower | upper | |||
| Knowledge About Ill Effects of FGM | ||||||
| Has Knowledge | 68 | 15 | ||||
| No Knowledge | 19 | 98 | 23.38 | 11.11 | 49.22 | < 0.001 |
| Mother Circumcision Status | ||||||
| Not Circumcised | 47 | 3 | ||||
| Circumcised | 40 | 110 | 43.08 | 12.69 | 146.22 | < 0.001 |
| Attitude towards FGM | ||||||
| Negative | 82 | 9 | ||||
| Positive | 5 | 104 | 189.51 | 61.16 | 587.18 | < 0.001 |
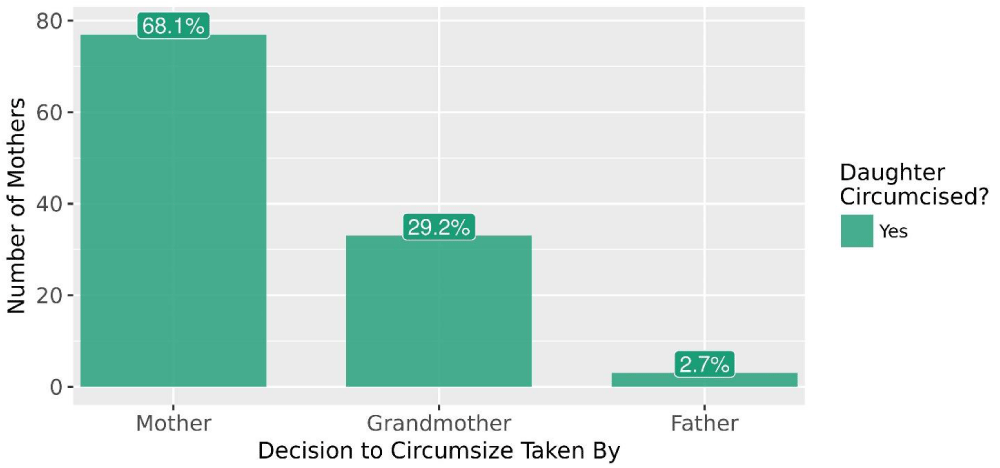
Figure 1: Barplot showing who took decision to circumcise the daughter.
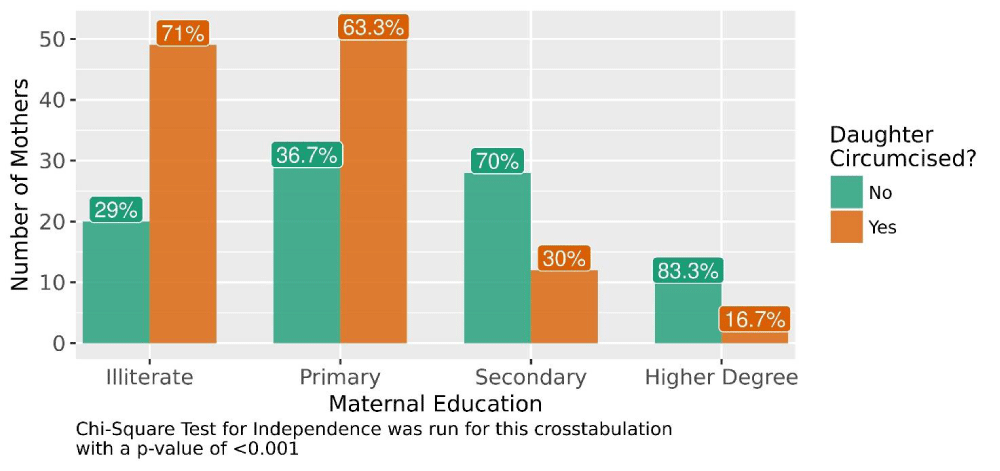
Figure 2: Barplot demonstrating the association between Maternal Education and daughter circumcision.
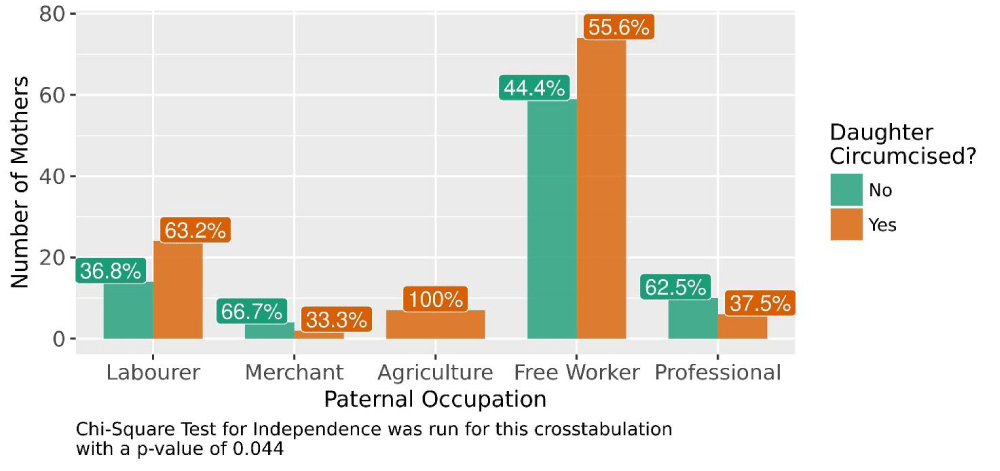
Figure 3: Barplot demonstrating the association between Father Occupation and daughter circumcision.
Binary logistic regression
All variables that were statistically significantly associated to FGM (including socio-demographics) were entered as predictors into a regression model of binary logistic family to assess which was independently associated with FGM was an Outcome variable.
Multiple Models were run, the table 3 is most accurate model obtainable. As evident, more modest Odd Ratios were obtained when compared to singular tests of associations.
| Table 3: Binary Logistic Regression. | ||||
| 95% CI of OR | ||||
| Factor | OR | 2.5% | 97.5% | p - value |
| Maternal Circumcision Status | 14.03 | 2.81 | 95.45 | < 0.001 |
| Attitude towards FGM | 48.53 | 14.45 | 198.69 | < 0.001 |
| Lack of Knowledge of Ill effects | 4.29 | 1.13 | 15.37 | 0.03 |
The practice of female genital cutting is a very deeply rooted harmful tradition that dates back centuries in most African and some Arabian countries [15].
This study attempted to assess factors associated with female circumcision among daughters of reproductive aged women in ACTH, Khartoum. In this study, 56.5% had at least one circumcised daughter. This finding is lower than the studies conducted in Egypt (77.3 %) [19] and East Gojjam Zone, Ethiopia (62.7%) [14]. However, it is higher when compared to study conducted in Somali refugees in Ethiopia (42.4%) [10] and in Hababo Guduru district (48%) [16]. These differences might be due to differences in place of the studies that might be explained by different strategies in combating FGM and different attitude level of the respondents about FGM. The other possible explanation could be the difference in cultural background of the study participants.
In this study, 75% of the mothers were circumcised. This is similar to the study done in Northwest Ethiopia (77%) However, this figure is significantly lower than the prevalence of studies done Hababo Guduru, Eastern Ethiopia and Amhara [10,14,16] but higher than the findings in Burkina Faso (68.1%)[11].
Circumcised women were significantly associated with daughters genital cutting practices in this study compared to non-circumcised women. 73% of circumcised mothers had at least one circumcised daughter compared to only 6% of non-circumcised mothers that circumcised their daughters. This is in line with other studies done in Iraq [20] and Ethiopia [27].
Knowledge about health ill effects of FGM was significantly associated with the daughters’ circumcision status. Mothers who had a good level of knowledge about FGM had less odds of having circumcised daughters as compared to those who had a poor level of knowledge. Furthermore, the study found attitude as another factor influencing FGM. Female genital mutilation was significantly higher among mothers who had a negative attitude as compared to those who had a positive attitude. This is in line with the studies done in Egypt [21] and Ethiopia [22].
Educational status and age had shown statistically significant association with female genital cutting practices in this study. Individuals with educational status of primary and above were less likely to practice than those who were illiterate. This finding is in line with other studies done in Iran [13] and Ethiopia [23]. Age of mothers is one of the factors determining to have circumcised daughters, mothers that circumcised their daughters had a higher mean age than those that didn’t. This might be explained by young mothers are closer to information and FGM is being discouraged. This is in line with the study done in Debaytilatgin district [15] and Hababo Guduru district [16].
Residence and origin of mothers also significantly affects the daughters’ circumcision status. 89% of mother residing in rural area had at least of circumcised daughter compared to only 51% in urban areas. This is in line with UNICEF publications [24] and studies done in Egypt [25].
Religion of the parents was another factor influencing daughter’s circumcision, where only 2% of Christians circumcised their daughters. This finding is consistent with the study conducted in Upper Egypt [19] and Burkina Faso [26]. There were no significant association between maternal occupation and FGM.
Socioeconomic status is also one of the factors determining daughter’s circumcision. This is consistent with another study conducted in Sudan [27] and Ethiopia [12].
FGM practice is still high in Sudan.
Age, Socio-economic status, Educational level, residence, origin, maternal circumcision status, Knowledge of ill effects and attitude towards FGM were all found to be associated with the decision to circumcise daughters.
The results of this study suggest the need for comprehensive and intensified community based efforts in the rural and high FGM practice clustered regions of Sudan.
Governmental and non-governmental organizations should work towards building a community of girls free from this harmful traditional practice by increasing awareness, media coverage and health education. Giving attention to mothers living in rural areas, taking necessary measurement on traditional circumcisers, working with religious leaders, alerting the community that FGM is a crime and giving awareness about the ill effects of FGM is strongly recommended.
Mother’s education was found to be significantly associated with FGM so this suggests the need for the government to provide and improve female education in Sudan.
It is also of great importance for the government to provide a National legislation prohibiting FGM in Sudan, in which those who fail to follow are subjected to great consequences.
Finally, further research is recommended to be conducted in different parts of Sudan to accurately address the reasons leading to the persistence of FGM and a larger number of Christians should participate in future studies.
Declaration
I, Danyah Shiddo, the undersigned, declare that the thesis is my original work and has not been presented for a degree at the University or any other university.
First and foremost, I would like to thank Allah SWT for giving me the strength, knowledge and opportunity to complete this research. Without His blessings, this achievement would not have been possible.
I would like to express my deep and sincere gratitude to my research supervisor, Dr. Hilmi Nour for his constant support, guidance and encouragement throughout these past few months.
I am also grateful to the staff of Academy Teaching Charity Hospital and the Obstetrics and Gynaecology unit for letting me carry out this research.
Most importantly, I would like to thank my parents and siblings, whose love and guidance are with me in whatever I pursue and especially my father, Dr. Ahmed Shiddo, thank you for being my mentor, my biggest inspiration and my role model, I couldn’t have done this without you.
- Prevalence of female genital mutilation. 2021. http://www.who.int/reproductivehealth/topics/fgm/prevalence/en/Female genital mutilation. 2021. http://www.who.int/mediacentre/factsheets/fs241/en/
- Female genital mutilation (FGM) frequently asked questions. 2021. https://www.unfpa.org/resources/female-genital-mutilation-fgm-frequently-asked-questions#where_practiced
- Female genital mutilation/cutting country profile. 2021. https://reliefweb.int/sites/reliefweb.int/files/resources/FGMC_SDN_Profile.pdf
- 2021. PubMed: https://www.unicef.org/protection/sudan_71891.html
- Islam M, Uddin M. Female Circumcision in Sudan: Future Prospects and Strategies for Eradication. International Family Planning Perspectives. 2021; 27: 71.
- 2021. http://www.refworld.org/pdfid/54bce53d4.pdf
- Health risks of female genital mutilation (FGM). 2021. https://www.who.int/teams/sexual-and-reproductive-health-and-research/areas-of-work/female-genital-mutilation/health-risks-of-female-genital-mutilation
- Satti A, Elmusharaf S, Bedri H, Idris T, Hashim M, et al. Prevalence and determinants of the practice of genital mutilation of girls in Khartoum, Sudan. Ann Trop Paediatr. 2006; 26: 303-310. PubMed: https://pubmed.ncbi.nlm.nih.gov/17132295/
- Mitike G, Deressa W. Prevalence and associated factors of female genital mutilation among Somali refugees in eastern Ethiopia: a cross-sectional study. BMC Public Health. 2009; 9: 264. PubMed: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2724517/
- Inungu J, Tou Y. Factors associated with female genital mutilation in Burkina Faso. J Public Health Epidemiol. 2013; 5: 20-28.
- Setegn T, Lakew Y, Deribe K. Geographic Variation and Factors Associated with Female Genital Mutilation among Reproductive Age Women in Ethiopia: A National Population Based Survey. PLoS One. 2016; 11: e0145329. PubMed: https://pubmed.ncbi.nlm.nih.gov/26741488/
- Pashaei T, Rahimi A. Related Factors of Female Genital Mutilation (FGM) in Ravansar (Iran). J Women's Health Care. 2012; 01.
- Mulusew A. Female Genital Mutilation and Associated Factors in GonchaSiso-Enessie District, East Gojjam Zone, Amhara Region, Ethiopia (2012). J Health Med Informat. 2013; 04.
- Ejigu Y, Tiruneh G, Kibret GD. Prevalence and Contributing Factors of Female Genital Cutting in Debaytilatgin District, Northwest Ethiopia. Clin Mother Child Health. 2014; 11.
- Gajaa M, Wakgari N, Kebede Y, Derseh L. Prevalence and associated factors of circumcision among daughters of reproductive aged women in the Hababo Guduru District, Western Ethiopia: a cross-sectional study. BMC Women's Health. 2016; 16.
- Desalegn S, Negussie D, Gamachu F, Tadele K, Markos D. Prevalence and associated factors of female genital mutilation among high school students in Dale Wabera Woreda, Oromia Regional State, Ethiopia. Int J Med Med Sci. 2017; 9: 72-78.
- Emam E, El-maghawry AM, Labeeb SA. Cultural Awareness about Female Genital Mutilation among Female Employees of Minia University. J Am Sci. 2011; 7.
- Shabila N. Mothers ’ factors associated with female genital mutilation in daughters in the Iraqi Kurdistan Region. Women Health. 2016; 57: 283-294. PubMed: https://pubmed.ncbi.nlm.nih.gov/26984379/
- Dalal K, Lawoko S, Jansson B. Women's attitudes towards discontinuation of female genital mutilation in Egypt. J Inj Violence Res. 2010; 2: 41-47. PubMed: https://pubmed.ncbi.nlm.nih.gov/21483197/
- Gebremariam K, Assefa D, Weldegebreal F. Prevalence and associated factors of female genital cutting among young adult females in Jigjiga district, eastern Ethiopia: a cross-sectional mixed study. Int J Womens Health. 2016; 8: 357-365. PubMed: https://pubmed.ncbi.nlm.nih.gov/27563257/
- Fikrie Z. Factors associated with perceived continuation of females ’ genital mutilation among women in Ethiopia. Ethiopian J Health Sci. 2011; 20: 49-53. PubMed: https://pubmed.ncbi.nlm.nih.gov/22434960/
- UNICEF publications. Unicef.org. 2021. PubMed: https://www.unicef.org/publications/files/FGM-C_final_10_October.pdf
- Van Rossem R, Meekers D, Gage A. Trends in attitudes towards female genital mutilation among ever-married Egyptian women, evidence from the Demographic and Health Surveys, 1995–2014: paths of change. Int J Equity Health. 2016, 15: 31. PubMed: https://pubmed.ncbi.nlm.nih.gov/26911243/
- Hayford S, Trinitapoli J. Religious Differences in Female Genital Cutting: A Case Study from Burkina Faso. J Sci Study Relig. 2011, 50: 252-271. PubMed: https://pubmed.ncbi.nlm.nih.gov/21969936/
- Ismail HS. Factors Influencing the Continuation of Female Genital Mutilation/Cutting Practice in Sudan. 2012.
- Azeze G, Williams A, Tweya H, Obsa M, Mokonnon T, et al. Changing prevalence and factors associated with female genital mutilation in Ethiopia: Data from the 2000, 2005 and 2016 national demographic health surveys. PLoS One. 2020; 15: e0238495. PubMed: https://pubmed.ncbi.nlm.nih.gov/32881931/